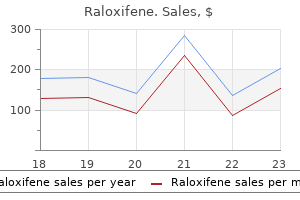
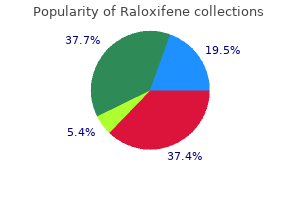
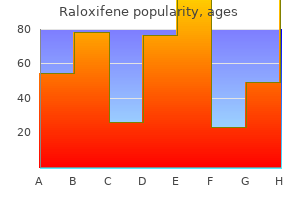
Raloxifene
Raloxifene dosages: 60 mg
Raloxifene packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Generic raloxifene 60 mg
Changes in plasma lipids and lipoproteins in overweight men during weight loss through dieting as compared with exercise women's health center san bernardino purchase online raloxifene. A meta-analysis of the past 25 years of weight loss research using diet, exercise or diet plus exercise intervention. Prevention of type 2 (non-insulindependent) diabetes by diet and physical exercise. Preoperative weight gain does not predict failure of weight loss or co-morbidity resolution of laparoscopic Roux-en-Y gastric bypass for morbid obesity. Effect of preoperative weight loss in bariatric surgical patients: a systematic review. Ten and more years after vertical banded gastroplasty as primary operation for morbid obesity. An experimental evaluation of the nutritional importance of proximal and distal small intestine. A prospective comparison of gastric and jejunoileal bypass procedures for morbid obesity. Weight loss and dietary intake after vertical banded gastroplasty and Roux-enY gastric bypass. Laparoscopic adjustable silicone gastric banding in the treatment of morbid obesity. Assessment of predictive ability of Epworth scoring in screening of patients with sleep apnoea. The place of upper gastrointestinal tract endoscopy before and after vertical banded gastroplasty for morbid obesity. Flexible endoscopy in the management of patients undergoing Roux-en-Y gastric bypass. Risks and benefits of prophylactic inferior vena cava filters in patients undergoing bariatric surgery. Safety and efficacy of simultaneous cholecystectomy at the time of Roux-en-Y gastric bypass. A multicenter, placebo-controlled, randomized, double-blind prospective trial of prophylactic ursodiol for the prevention of gallstone formation following gastric-bypass-induced rapid weight loss. Preoperative weight loss in high-risk superobese bariatric patients: a computed tomography-based analysis. Laparoscopic versus open gastric bypass: a randomized study of outcomes, quality of life, and costs. A multicenter, prospective, risk-adjusted analysis from the National Surgical Quality Improvement Program. Open versus laparoscopic Roux-en-Y gastric bypass: a comparative study of over 25,000 open cases and the major laparoscopic bariatric reported series.
Buy raloxifene amex
Iatrogenic small bowel perforation incurred during endoscopy womens health redding ca buy genuine raloxifene on-line, if immediately recognized, can sometimes be repaired using endoscopic techniques. Perforation of the jejunum and ileum occurs into the peritoneal cavity and usually causes overt symptoms and signs, such as abdominal pain, tenderness, and distention accompanied by fever and tachycardia. Plain abdominal radiographs may reveal free intraperitoneal air if intraperitoneal perforation has occurred. Chylous Ascites Chylous ascites refers to the accumulation of triglyceride-rich peritoneal fluid with a milky or creamy appearance, caused by the presence of intestinal lymph in the peritoneal cavity. Chylomicrons, produced by the intestine and secreted into lymph during the absorption of long-chain fatty acids, account for the characteristic appearance and triglyceride content of chyle. The most common etiologies of chylous ascites in Western countries are abdominal malignancies and cirrhosis. In Eastern and developing countries, infectious etiologies, such as tuberculosis and filariasis, account for most cases. Chylous ascites can also develop as a complication of abdominal and thoracic operations and trauma. Operations particularly associated with this complication include abdominal aortic aneurysm repair, retroperitoneal lymph node dissection, inferior vena cava resection, and liver transplantation. Other etiologies of chylous ascites include congenital lymphatic abnormalities. Three mechanisms have been postulated to cause chylous ascites: (a) exudation of chyle from dilated lymphatics on the wall of the bowel and in the mesentery caused by obstruction of lymphatic vessels at the base of the mesentery or the cisterna chili. Patients with chylous ascites develop abdominal distention over a period of weeks to months. Postoperative chylous ascites can present acutely during the first postoperative week. Delayed presentations following surgery can occur if the mechanism of ascites formation is adhesion-induced lymphatic obstruction rather than lymphatic vessel disruption. Chyle typically has a cloudy and turbid appearance; however, it may be clear in fasting patients (such as those in the immediate postoperative period). Lymphangiography and lymphoscintigraphy may help localize lymph leaks and obstruction; this information is particularly useful for surgical planning. The general approach is to focus on evaluating and treating the underlying causes, especially for patients with infectious, inflammatory, or hemodynamic etiologies for this condition. Most patients respond to administration of a high-protein and low-fat diet supplemented with medium-chain triglycerides.
Raloxifene 60 mg buy with amex
The use of laparoscopy in the elderly has significantly increased in recent years menstrual cramps buy 60 mg raloxifene. In general, laparoscopic appendectomy offers elderly patients with appendicitis a shorter length of hospital stay, a reduction in complication and mortality rates, and a greater chance of discharge to home (independent of further nursing care or rehabilitation). Acute appendicitis can occur at any time during pregnancy but is rare in the third trimester. The diversity of clinical presentations and the difficulty in making the diagnosis of acute appendicitis in pregnant women are well established. This is particularly true in the late second trimester and the third trimester, when many abdominal symptoms may be considered pregnancy related. In addition, during pregnancy, there are anatomic changes in the appendix and increased abdominal laxity that may further complicate clinical evaluation. Appendicitis in pregnancy should be suspected when a pregnant woman complains of abdominal pain of new onset. The most consistent sign encountered in acute appendicitis during pregnancy is pain in the right side of the abdomen. Seventy-four percent of patients report pain located in the right lower abdominal quadrant, with no difference between early and late pregnancy. Only 57% of patients present with the classic history of diffuse periumbilical pain migrating to the right lower quadrant. Laboratory evaluation is not helpful in establishing the diagnosis of acute appendicitis during pregnancy. The physiologic leukocytosis of pregnancy has been defined as high as 16,000 cells/mm3. In one series, only 38% of patients with appendicitis had a white blood cell count of more than 16,000 cells/mm3. Another option is magnetic resonance imaging, which has no known deleterious effects on the fetus. The American College of Radiology recommends the use of nonionizing radiation techniques for front-line imaging in Acute Appendicitis during Pregnancy pregnant women. In an analysis of outcomes in California using administrative databases, laparoscopy was found to be associated with a 2. Rates of fetal loss are considerably higher in women with complicated appendicitis than in those with a negative appendectomy or with simple appendicitis. Removing a normal appendix is associated with a 4% risk of fetal loss and 10% risk of early delivery. Because the incidence of complicated appendix is similar in pregnant and nonpregnant women and because maternal mortality is so low, it appears that the greatest opportunity to improve fetal outcomes is by improving diagnostic accuracy and reducing the rate of negative appendectomy. Patients presenting with stump appendicitis are more likely to have complicated appendicitis, have an open procedure, and undergo colectomy. In patients who have had prior appendectomy, a low index of suspicion is important to prevent delay in diagnosis and complications.
Discount raloxifene 60 mg on-line
A limited women's health clinic des moines iowa generic raloxifene 60 mg on line, highly selective proximal gastric vagotomy is performed along the cephalad 4 cm of the lesser curvature. A neck incision is made along the anterior border of the left sternocleidomastoid muscle, and the strap muscles are exposed. The omohyoid muscle is divided at its pulley, and the sternohyoid and sternothyroid muscles are divided at their manubrial insertion. The left carotid sheath is retracted laterally and the thyroid and trachea medially. The left inferior thyroid artery is ligated laterally as it passes under the left common carotid artery. The esophagus is dissected circumferentially in an inferior direction, from the left neck to the apex of the right chest, to avoid injury to the right recurrent laryngeal nerve. The esophagus is divided at the level of the thoracic inlet, leaving about 3 to 4 cm of cervical esophagus. The proximal esophagus is retracted anteriorly and to the right with the use of two sutures to keep saliva and oral contents from contaminating the neck wound. Returning to the abdomen, the proximal staple line of the gastric division is opened and the esophagus is flushed with povidone-iodine solution. The distal portion of the esophagus in the neck is secured tightly around the stripping cable with "endoloops" and an umbilical tape for a trailer. The tip of the stripper is exchanged for a mushroom head, and the stripper is pulled back into the abdomen, inverting the esophagus as it transverses the posterior mediastinum. This maneuver strips the branches of the esophageal plexus off the longitudinal muscle of the esophagus, preserving the esophageal plexus along with the proximal vagal nerves and the distal vagal nerve trunks. In patients with end-stage achalasia, only the mucosa is secured around the stripping cable, so that it alone is stripped and the dilated muscular wall of the esophagus, with its enriched blood supply, remains. The resulting mediastinal tunnel, or in the case of achalasia the muscular tube, is dilated with a Foley catheter containing 90 mL of fluid in the balloon. The previously prepared interposed portion of the transverse colon is passed behind the stomach and up through the mediastinal tunnel into the neck. An end-to-end anastomosis is performed to the cervical esophagus using a single layer technique. The colon is pulled taut and secured to the left crus with four or chaptEr 25 Esophagus and diaphragmatic hErnia 1026 five interrupted sutures. The proximal end, which is the distal end of the interposed colon, is anastomosed high on the posterior fundic wall of the stomach, using a triangular stapling anastomotic technique. Colonic continuity is re-established by bringing the proximal right colon to the distal staple line in the left colon and performing an end-to-end anastomosis using a double layer technique.
Raloxifene 60 mg purchase visa
Irritable bowel syndrome is a particularly troubling constellation of symptoms consisting of crampy abdominal pain womens health ukiah ca discount raloxifene 60 mg without prescription, bloating, constipation, and urgent diarrhea. Once other disorders have been excluded, dietary restrictions and avoidance of caffeine, alcohol, and tobacco may help to alleviate symptoms. The incidence of fecal incontinence has been estimated to occur in 10 to 13 individuals per 1000 people older than age 65 years. Incontinence ranges in severity from occasional leakage of gas and liquid stool to daily loss of solid stool. The underlying cause of incontinence is often multifactorial, and diarrhea is often contributory. Neurogenic causes include diseases of the central nervous system and spinal cord along with pudendal nerve injury. Anatomic causes include congenital abnormalities, procidentia (rectal prolapse), overflow incontinence secondary to impaction or an obstructing neoplasm, and trauma. The most common traumatic cause of incontinence is injury to the anal sphincter during vaginal delivery. After a thorough medical evaluation to detect underlying conditions that might contribute to incontinence, evaluation focuses on assessment of the anal sphincter and pudendal nerves. Even in the absence of frank diarrhea, the addition of dietary fiber may improve continence. Many patients with a sphincter defect are candidates for an overlapping sphincteroplasty. Innovative technologies such as sacral nerve stimulation and the artificial bowel sphincter are proving useful in patients who fail other interventions. Although the indication and urgency for surgery will alter some of the technical details, the operative principles of colorectal resections, anastomoses, and use of ostomies are well established. The mesenteric clearance technique dictates the extent of colonic resection and is determined by the nature of the primary pathology (malignant or benign), the intent of the resection (curative or palliative), the precise location(s) of the primary pathology, and the condition of the mesentery (thin and soft or thick and indurated). In general, a proximal mesenteric 1 ligation will eliminate the blood supply to a greater length of colon and require a more extensive "colectomy. Emergency resection may be required because of obstruction, perforation, or hemorrhage. The surgical principles described earlier apply, and an attempt should be made to resect the involved segment along with its lymphovascular supply. If the resection involves the right colon or proximal transverse colon (right or extended right colectomy), a primary ileocolonic anastomosis can usually be performed safely as long as the remaining bowel appears healthy and the patient is stable.
Cheap generic raloxifene canada
Despite the myriad of causes menstrual ovulation cycle calculator order on line raloxifene, the majority of pruritus ani is idiopathic and probably related to local hygiene, neurogenic, or Diagnosis. Patients describe symptoms varying from the sensation of passing flatus from the vagina to the passage of solid stool from the vagina. Large fistulas may be obvious on anoscopic and/or vaginal speculum examination, but smaller fistulas may be difficult to locate. Treatment focuses on removal of irritants, improving perianal hygiene, dietary adjustments, and avoiding scratching. Biopsy and/or culture may be required to rule out an infectious or dermatologic cause. Systemic antihistamines or tricyclic antidepressants have also been used with some success. Chlamydia trachomatis infection may be asymptomatic or may produce similar symptoms. Chancroid, caused by Haemophilus ducreyi, is a disease manifested by multiple painful, bleeding lesions. Donovania granulomatis infection produces shiny, red masses on the perineum (granuloma inguinale). Diarrheal illnesses caused by organisms such as Campylobacter or Shigella may also be sexually transmitted. Leprosy, amebiasis, actinomycosis, and lymphogranuloma venereum produce characteristic perianal lesions. Treatment consists of antimicrobial agents directed against the infecting organism. Amebas produce ulcerations in the gastrointestinal mucosa and can infect any part of the gut. Giardia lamblia is also common and produces diarrhea, abdominal pain, and malaise. Proctitis is usually caused by type 2 herpes simplex virus and less commonly by type 1 herpes simplex virus. Pain often precedes the development of characteristic vesicles, and these patients may require an examination under anesthesia to exclude another diagnosis such as an intersphincteric abscess. Condylomas occur in the perianal area or in the squamous epithelium of the anal canal. Small warts on the perianal skin and distal anal canal may be treated in the office with topical application of bichloracetic acid or podophyllin. Although 60% to 80% of patients will respond to these agents, recurrence and reinfection are common. Imiquimod (Aldara) is an immunomodulator that was recently introduced for topical treatment of several viral infections, including anogenital condyloma. Larger and/ or more numerous warts require excision and/or fulguration in the operating room. Excised warts should be sent for pathologic examination to rule out dysplasia or malignancy.
Cheap generic raloxifene uk
Algorithm used to facilitate decisions regarding treatment of acute aortic dissection menstruation rash raloxifene 60 mg. The thin and inflamed outer wall of a dissected ascending aorta often produces a serosanguineous pericardial effusion that can accumulate and cause tamponade. Free rupture into the pericardial space produces rapid tamponade and is generally fatal. As the dissection progresses, any branch vessel from the aorta can become involved, which results in compromised blood flow and ischemic complications. Therefore, depending on which arteries are involved, the dissection can produce acute stroke, paraplegia, hepatic failure, bowel infarction, renal failure, or a threatened ischemic limb. Diagnostic Evaluation Because of the variations in severity and the wide variety of potential clinical manifestations, the diagnosis of acute aortic dissection can be challenging. Not surprisingly, diagnostic delays are common; delays beyond 24 hours after hospitalization occur in up to 39% of cases. Unfortunately, delays in diagnosis lead to delays in treatment, which can have disastrous consequences. Most of the other common symptoms either are nonspecific or are caused by the secondary manifestations of dissection. A discrepancy between the extremities in pulse, blood pressure, or both is the classic physical finding in patients with aortic dissection. It often occurs because of changes in flow in the true and false lumens, and it does not necessarily indicate extension into an extremity branch vessel. Involvement of the aortic arch often creates differences between the right and left arms, whereas descending aortic dissection often causes differences between the upper and lower extremities. Like symptoms, most of the physical signs after dissection are related to the secondary manifestations and therefore vary considerably Table 22-5). For example, signs of stroke or a threatened ischemic limb may dominate the physical findings in patients with carotid or iliac malperfusion, respectively. Unfortunately, laboratory studies are of little help in diagnosing acute aortic dissection. There has been continued interest in using D-dimer level to aid in making this diagnosis. The accuracy of these noninvasive imaging tests has all but eliminated the need for diagnostic aortography in most patients with suspected aortic dissection. Computed tomographic scans showing that the aorta has been separated into two channels-the true (T) and false (F) lumens- in two patients with different phases of aortic dissection. Here, the true lumen of the proximal aorta can be seen to be extensively compressed. In the chronic phase, the membrane appears straighter and less mobile (arrow) because it has stabilized over time. Contraindications include hemodynamic instability, aortic rupture, and pericardial effusion.

Raloxifene 60 mg low cost
However menstruation cup raloxifene 60 mg buy with amex, one fourth will continue to bleed or will rebleed after an initial quiescent period, and virtually all the mortalities (and all the operations for bleeding) occur in this group. This group can be fairly well delineated based on clinical factors related to the magnitude of the hemorrhage, comorbidities, age, and endoscopic findings. Shock, hematemesis, transfusion requirement exceeding four units in 24 hours, and certain endoscopic stigmata (active bleeding or visible vessel) define this high-risk group. Two widely used risk stratification tools have proven useful in predicting rebleeding and death: the Blatchford and Rockall scores Table 26-9). The most common endoscopic hemostatic modalities used are injection with epinephrine, and electrocautery. In a case with exposed vessel, mechanical hemostasis using a clip is useful to control the bleeding. Elderly patients and patients with multiple comorbidities do not tolerate repeated episodes of hemodynamically significant hemorrhage, and may benefit from early elective operation after initially successful endoscopic treatment, especially if they have a high-risk ulcer. Planned surgery under controlled circumstances often yields better outcomes than emergent surgery. Deep bleeding ulcers on the posterior duodenal bulb or lesser gastric curvature are high-risk lesions, because they often erode large arteries not amenable to nonoperative treatment, and early operation should be considered. Complications 1060 Table 26-9 Risk-stratification tools for upper gastrointestinal hemorrhagea A. Panel B shows the Rockall score, with point values assigned for each of three clinical variables (age and the presence of shock and coexisting illnesses) and two endoscopic variables (diagnosis and stigmata of recent hemorrhage). The complete Rockall score ranges from 0 to 11, with higher scores indicating higher risk. Patients with a clinical Rockall score (Age + Shock + Coexisting illness) of 0 or a complete Rockall score of 2 or less are considered to be at low risk for rebleeding or death. The patient can often give the exact time of onset of the excruciating abdominal pain. Initially, a chemical peritonitis develops from the gastric and/or duodenal secretions, but within hours a bacterial peritonitis supervenes. The patient is in obvious distress, and the abdominal examination shows peritoneal signs. Usually, marked involuntary guarding and rebound tenderness is evoked by a gentle examination. Once the diagnosis has been made, the patient is given analgesia and antibiotics, resuscitated with isotonic fluid, and taken to the operating room. Fluid sequestration into the third space of the inflamed peritoneum can be impressive, so preoperative fluid resuscitation is mandatory. Sometimes, the perforation has sealed spontaneously by the time of presentation, and surgery can be avoided if the patient is doing well.
Keldron, 34 years: This is facilitated by dividing any loose areolar tissue overlying the ligamentum venosum, which is divided proximally. Surgical adhesive is used to obliterate the false lumen and strengthen the aorta for the distal anastomosis.
Snorre, 54 years: Usually, marked involuntary guarding and rebound tenderness is evoked by a gentle examination. In greater than 70% of patients, the disease is stable, particularly with risk factor modification.
Khabir, 59 years: Prokinetic agents, such as metoclopramide and erythromycin, are associated with poor efficacy. Comorbid medical problems may already be present in severely obese adolescents, including hypertension and type 2 diabetes.
Joey, 44 years: The signals are then processed to reconstruct multiple slices which together provide a three-dimensional view. Both oral and topical calcium channel blockers (diltiazem and nifedipine) have also been used to heal fissures and may have fewer side effects than topical nitrates.
Marius, 43 years: This method is most useful for graft punctures, patients with abnormal clotting profiles, or if thrombolytic therapy is anticipated. Historically, the recommendation was to avoid biopsy because of the risk of infection or needle tract seeding.
Kaffu, 53 years: The thoracic duct passes through the hiatus of the diaphragm on the anterior surface of the vertebral column behind the aorta and under the right crus. When endoscopic esophagitis is seen, severity and the length of esophagitis involved are recorded.
Barrack, 42 years: The circumference of the diaphragmatic hiatus is dissected and the esophagus is mobilized by careful dissection of the anterior and posterior soft tissues within the hiatus. Other authors have advocated a selective approach, with a recommendation to remove diverticula attached by bands and those with narrow bases, on the assumption that these diverticula are more likely to develop complications.
Kulak, 31 years: Prokinetic agents, such as metoclopramide and erythromycin, are associated with poor efficacy. It is hoped that the more gradual clot dissolution with thrombolysis may decrease the incidence of reperfusion injury that is encountered after open surgical procedures where rapid return of blood flow may precipitate compartment syndrome.
Kor-Shach, 51 years: Function following anterior resection is highly dependent on the level of anastomosis, the use of pre- or postoperative pelvic radiation, and underlying sphincter function. Internally, myxomas are heterogeneous and often contain hemorrhage, cysts, necrosis, or calcification.
Karmok, 37 years: Atherosclerotic lesions in other territories such as the coronary, mesenteric, cerebrovascular, and peripheral arterial circulation are common. It is usually seen in the pediatric population, where the cecum intussuscepts into the ileum (ileocolic intussusception).
Hamlar, 48 years: Moreover, some experimental data suggest that minimally invasive operations have less immunosuppressive impact on the patient and thus might improve postoperative outcome and even long-term survival. If an antecolic route is to be used, the end of the Roux limb is brought up so as to confirm its ability to reach the stomach.
Gunock, 47 years: Prognosis of aortic intramural hematoma with and without penetrating atherosclerotic ulcer: a clinical and radiological analysis. The success rate for the severely obese patient population that tries dieting and exercise as a means of losing enough weight to no longer be obese and maintaining that weight loss is only approximately 3%.
9 of 10 - Review by E. Ortega
Votes: 30 votes
Total customer reviews: 30