Tofranil
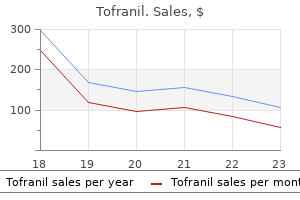
Tofranil dosages: 75 mg, 50 mg, 25 mg
Tofranil packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

25 mg tofranil fast delivery
Educational materials backed by an honest but positive and confident approach during the explanation session are important in successfully achieving the goals of a transesophageal study in an older child or adolescent anxiety disorder nos 3000 safe 75 mg tofranil. In infants and small children, the same approach is modified and directed toward the parents. Sedation If general anesthesia is not being used as described above, mild to moderate sedation usually is sufficient to maximize patient cooperation while relieving discomfort and anxiety. Premature atrial extrastimulus technique (during sinus and/or eight-beat drives of a-paced rhythm) 3. Premature atrial extrastimulus technique (during sinus and/or eight-beat drives of a-paced rhythm) 5. Premature ventricular extrastimulus technique (during eight-beat drives of v-paced rhythm) 6. Continuous atrial decremental pacing (or short bursts) to determine minimum cycle length for 1:1 conduction in the accessory pathway c. Premature right ventricular extrastimulus technique (using one or more drive cycle lengths) to determine the presence of retrograde conduction and the effective refractory of the accessory pathway. Preparation of Patient in the Procedure Room Whether in an inpatient or outpatient setting, the transesophageal technique is adaptable to virtually any type of room or location where the patient can be comfortably supine and where sufficient space exists for equipment and monitoring. Sedation is administered as needed with appropriate vital sign (heart rate, respiratory rate, and blood pressure) and oximetry monitoring protocols established. In most infants and children, comfortable extremity restraints are necessary to prevent withdrawal of the catheter by the patient. A soothing, comforting manner is necessary for successful passage of the catheter, as well as for successful recording and stimulation because of the potential mild discomfort encountered during each of these steps. The distance of catheter advancement required to reach the predicted area best suited for recording and pacing directly correlates with patient height (40). However, this predicted depth may not actually be the ideal location, and minor adjustments may be necessary. The optimal catheter electrode position for pacing correlates with the highest atrial electrogram amplitude. Short distances (a few millimeters) of catheter withdrawal and advancement are performed until the maximum atrial electrogram amplitude is found. Successful transesophageal recording and stimulation in infants, children, and adolescents have been reported with various types of electrode catheters. Although the adult "pill" electrode can be used in the older child and adolescent, the electrode catheter is better suited for the pediatric patient. Interelectrode distance (12, 22, and 28 mm) was found to have no significant effect on pacing thresholds regardless of age or size of the patient (32,36,40,41). Essentially no data are available that compare catheter sizes in pediatric patients; however, intuitively, if electrode contact with the esophageal wall is an important goal, the largest possible catheter size should be used.
50 mg tofranil purchase free shipping
These injuries are underdiagnosed because chest pain associated with blunt chest injury is often attributed to concomitant chest wall contusion anxiety symptoms during pregnancy order tofranil us, pericarditis, pulmonary contusion, rib fractures, or other associated injuries that are not routinely evaluated by coronary angiography. Coronary angiography is indicated for all blunt cardiac trauma patients with angina or myocardial infarction to determine the status of the coronary arteries and to locate surgically correctable lesions. Penetrating Cardiac Injury Although blunt trauma accounts for most injuries among the pediatric population, penetrating trauma is increasing among young adults, teenagers, and even younger children. It was common wisdom for years that nothing could be done for wounds to the heart until von Rehn performed the first successful cardiorrhaphy in 1896 for a 22-year-old man with a 1. Theodore Billroth that, "A surgeon who tries to suture a wound of the heart deserves to lose the esteem of his colleagues" (41). The mortality risk for penetrating cardiac trauma is related to a number of factors, including the cause of injury, size of the wound, location of the wound, any associated noncardiac injuries, and length of time from injury to initiation of resuscitative measures. Not only does a bullet cause greater disruption of myocardium and internal structures of the heart, but the rent in the pericardium is larger, which makes tamponade less likely and exsanguination more rapid. For these reasons, the mortality rate of gunshot wounds to the heart is approximately twice that of stab wounds. However, if allowed to progress, hemopericardium can lead to fatal cardiac tamponade. Because of its thicker myocardial wall, stab wounds to the left ventricle that measure <1 cm will often spontaneously seal. Stab wounds to the right ventricular wall, however, usually result in cardiac tamponade because the thinner myocardial wall does not usually spontaneously seal. As is the case with blunt cardiac trauma, the anatomic position of cardiac structures determines their likelihood of injury owing to penetrating trauma. Other causes of penetrating injury to the heart include ice picks, nonbullet projectiles, swallowed sewing needles, and inward displacement of fractured ribs with chest trauma (44). Beck triad is frequently absent in patients with cardiac tamponade, and determination of jugular venous distension is particularly difficult in young children because of their short necks. In addition, if there is hypovolemia owing to acute blood loss, increased central venous pressure may not be seen with cardiac tamponade (41). Ten percent to thirty percent of patients with penetrating cardiac wounds also have intra-abdominal injury. This is important because mortality is greater for patients with penetrating cardiac injury associated with intra-abdominal injury than for those with cardiac injury alone (41). Emergency department echocardiography is available at some trauma centers, which has decreased the time to diagnosis of penetrating cardiac injury and has improved survival. Pericardiocentesis can rule in, but not rule out, cardiac tamponade because of the high frequency of falsenegative P. Performing a subxiphoid pericardial window has been recommended by some to diagnose hemopericardium in selected stable trauma patients.
Discount tofranil 25 mg buy
Echocardiographers must resist the tendency to become less rigorous when performing the echocardiographic examination because other imaging modalities exist as bailout options anxiety relief tofranil 75 mg order mastercard. If complex, difficult anatomy is possible to be diagnosed by echocardiography, the echocardiographer should make every attempt to do so in order to avoid the expense, inconvenience, and potential risk associated with other imaging modalities. Echocardiography personnel need to continue to bring the same rigor and compulsiveness to the examination that were employed in the past. The second challenge is one of "imaging responsibility" to not only patients and but also the healthcare system. Cardiologists are responsible for recognizing and resisting the lure of employing all of the diagnostic armamentarium at their disposal. Echocardiographers need to lead the charge by partnering with colleagues from other imaging modalities to develop pathways for diagnostic approaches that are age- and disease-specific and bring the greatest value to the patient. Another challenge involves the increasing miniaturization of computer and ultrasound equipment. This trend has provided the exciting development of hand-carried ultrasound devices. Using such devices, cardiologists may be able to provide point-of-service care more effectively and frequently. Evidence shows that these devices also improve diagnostic accuracy by complementing the cardiac physical examination (113,114,115,116). However, the increased availability of echocardiography made possible by hand-carried devices has tempted other noncardiac specialists to practice cardiac ultrasound (117,118). It is the duty of the echocardiography community to develop standards for the practice of handcarried ultrasound and ensure that they are met. Most physicians who use a stethoscope are not cardiologists, the diagnostic accuracy P. A pediatrician may hear a murmur but may not be able to determine its etiology and therefore refers the patient to a pediatric cardiologist who will not only hear the murmur but will offer a definitive diagnosis. As with the stethoscope, it should be expected and indoctrinated as standard of care, that when a noncardiologist identifies a patient with suspected pathology using a hand-held device, the patient be referred to a cardiologist for further and definitive echocardiographic evaluation. Lastly, echocardiographers are taking more advantage of tele- and web-based technologies to expand their echocardiographic services and expertise to patients that normally may not be able to receive them. In addition, web-based networks allow reading echocardiograms from remote sites (119). Acquiring and reading echocardiograms with web-based technology has had a profound impact on more timely diagnosis of critically ill patients, better determination of need for cardiology consultation, and prevention of unnecessary transfers (120,121,122). These technologies require monitoring because they often involve quality assurance issues. The studies are usually not performed by pediatric-certified sonographers and the images may undergo some degradation. In addition, transmission speeds are sometimes too slow to employ a live image review which may result in patient inconvenience and diagnostic errors. Quality assurance processes are essential when developing a tele- or web-based echocardiography program.
Cheap tofranil 50 mg buy online
Poxvirus virions are large anxiety guru generic 75 mg tofranil amex, have a very complex structure, and are enveloped, but their envelope is not required for their virions to be infectious. Instead, replication of viruses requires certain host cell genes, proteins, and organelles. The viral replication cycle involves several steps: adsorption, cellular uptake, uncoating, biosynthesis, virion assembly, and release. The specificity of this interaction between the viral protein and host receptor defines and limits the species and cell type that a particular virus can infect. Alternately some viruses may enter the cell through invagination of the cell membrane forming vesicles in the cell cytoplasm. Nucleus (Nuc) of a stratum corneum cell, filled with papillomavirus virions (V); chromatin is marginated (M). Early viral proteins are usually nonstructural and may code for important enzymes, while later proteins tend to be structural components for the virion. This may occur in the nucleus, as it does with herpes viruses, or in the cytoplasm with polioviruses, or even at the cell surface with viruses such as influenza. The virions of most viruses, including papillomaviruses, herpesviruses, and poxviruses, are released upon cell lysis. Cytoplasm of a spinosum cell filled with mature molluscum contagiosum virions (V), immature virus forms (i), and viroplasm in a gyrate pattern (G). This can occur when virus proteins and nucleic acid condense adjacent to the cell membrane with subsequent budding off of the cell. Typically, hundreds or thousands of new virions are produced from each infected cell, which can then go on to infect other cells. One cycle of viral replication may last from 3 to 36 hours, depending on the virus and cell type involved. Interruption of any step in viral cellular entry, uncoating, synthesis, assembly, or release may prevent the development of new infectious virions. Viruses can also establish several alternate pathways in the host cell, discussed further in the next section. Human papillomaviruses can productively infect a very narrow range of cells, namely, certain differentiating human epidermal cells. However certain enveloped viruses can replicate without causing irreversible damage to the host cell. In noncytocidal infections other possible interactions with the host cell are persistent infection, viral latency, and tumor transformation. Latently infected cells either produce very small numbers of new virions so that spread to uninfected cells is minimal or they synthesize no virions but retain an intact and potentially inducible viral genome. Papillomaviruses similarly can encode nonvirion proteins that increase cell growth and lead to inappropriate control of cell division. The viral infectious nature of specific tumors has important implications for prevention, diagnosis, and therapy.
Best 75 mg tofranil
The right ventricle can also be identified by its coarse trabeculations along the septum and free wall anxiety 05 mg purchase generic tofranil from india. One of these trabeculations, the moderator band, is particularly prominent, running transversely from free wall to septum in the inferior third of the right ventricular cavity in the apical view. Once ventricular morphology has been established, ventricular looping is determined. This is performed by imagining one is standing in the right ventricle facing the right ventricular side of the interventricular septum and placing an imaginary hand on the ventricular septum. The looping is determined by which of the two hands allows the palm to lie on the septum, the thumb to point into the atrioventricular valve and the fingers to point into the outflow tract. In ventricular D-loop, the palm of the right hand is placed over the septum with the thumb in the tricuspid valve and the fingers in the right ventricular outflow tract. In ventricular L-loop, the palm of the left hand is placed over the septum with the thumb in the inflow and the fingers in the right ventricular outflow tract. Right Ventricle the size of the right ventricle and its relative contribution to the ventricular apex in conditions such as complete atrioventricular P. F: Straddling (atrioventricular valve attachments cross ventricular septum into the contralateral ventricle. G: Overriding (atrioventricular annulus overrides the ventricular septum so that it is partially committed to the contralateral ventricle but without attachments into the contralateral ventricle). H: Crisscross (atrioventricular valves are oriented more perpendicular to one another existing in either a concordant (shown) or discordant relationship to the ventricles). The tricuspid valve has chordal attachments to the ventricular septum (solid arrow in A) whereas the mitral valve does not (outlined arrow in A). These anatomic findings are used to determine complex ventricular relationships since the atrioventricular valve is associated with its respective ventricle. For example, in B, the left-sided atrioventricular valve has attachments to the ventricular septum, whereas the right-sided valve does not, allowing diagnosis of a left-sided tricuspid valve and a right sided mitral valve. The moderator band is near the apex of the left-sided ventricle, further defining this ventricle as a morphologic right ventricle because of ventricular inversion. Ventricular Septum the ventricular septum is composed of two components: (a) the membranous septum, which is an extremely small (5 mm in diameter in the adult heart) and superior portion wedged between the tricuspid and aortic valves; and (b) the large muscular septum. The muscular septum consists of three portions: the inlet portion, which is inferior to the membranous septum and is between the atrioventricular valves; the trabecular portion, which extends from the membranous septum to the apex; and the conal (or outlet or infundibular) septum, immediately below the pulmonary valve. The membranous septum is seen well in the parasternal long-axis sweep from the standard view toward the tricuspid valve. In the apical view, the transducer can be swept anteriorly toward the left ventricular outflow tract and aorta to visualize this portion of the septum. The trabecular septum is so large that defects within it need to be localized preferably describing their position in two orthogonal planes and in relation to nearby landmarks. The five leaflets of the common atrioventricular valve are shown including the superior and inferior bridging leaflets.
Buy tofranil discount
The association of supravalvar aortic stenosis anxiety symptoms in 9 year old discount 50 mg tofranil overnight delivery, multiple peripheral pulmonary artery stenosis, mental retardation, and peculiar facies has been described as Williams syndrome (107). Although rare, familial and nonfamilial cases of isolated peripheral pulmonary stenosis with no underlying syndrome also have been described (108). Embryology and Pathology the pulmonary artery and its branches developmentally have their origin from three separate vascular components. The proximal portion of the main pulmonary artery just above the semilunar valve probably is derived from the bulbus cordis. The peripheral portions of the pulmonary artery branches derive from the postbranchial pulmonary vascular plexus, which lies in close relationship to the growing lung buds. The pathogenesis of peripheral pulmonary artery stenosis is not completely understood but probably differs with the underlying process. At least one such agent, the rubella virus, appears to exert its teratogenic effect by interfering with the normal formation of the elastic tissues. Specific genetic abnormalities underlying many of the syndromes associated with isolated peripheral pulmonary artery stenosis are being increasingly recognized. A genetic deletion mapped to chromosome 7 resulting in abnormal elastin production was found in most patients with Williams syndrome (109). A deletion in chromosome 20 appears to be responsible for Alagille syndrome, but the resulting biochemical abnormality has not been identified (110). Several families with multiple relatives affected with Noonan syndrome have had the genetic mutation mapped to chromosome 12, and missense mutations in a specific gene on this chromosome are now known to account for more than 50% of cases (9,111). A useful classification of peripheral pulmonary artery stenosis was proposed by Gay et al. They classified the stenoses into four types: stenoses involving the main pulmonary trunk or the right and left branches, stenoses involving the bifurcation of the pulmonary artery extending into both branches, multiple peripheral stenoses, and a combination of main and peripheral stenoses. With long-segment constrictions, only minimal poststenotic dilation, if any, is seen, and no dilation at all is noted with the hypoplastic form. Physiology the physiology associated with peripheral pulmonary artery stenosis results in elevations of right ventricular and pulmonary artery (proximal to stenosis) systolic pressure that depends on the severity and distribution of the stenoses. In most cases, the obstruction is central and results in a limited volume capacity of the pulmonary trunk proximal to the obstruction. This explains the delay in pulmonary valve closure despite the high systolic pressure in the pulmonary tree. In cases of severe multiple peripheral pulmonary stenoses involving many small branches, closure of the pulmonary valve occurs early and approximates closure of the aortic valve. When the stenosis is unilateral and there is no left-toright shunt, resting right ventricular pressure remains normal. Measurement of flow distribution, rather than pressure gradients, is the best way to assess relative stenosis in the pulmonary branches. Manifestations Clinical Features Patients with mild or moderate bilateral pulmonary artery stenosis, as well as those with unilateral stenosis, are usually asymptomatic.
Discount tofranil 75 mg online
Anomalies of the Ductus Venosus Anomalous Termination of the Umbilical Veins and Absent Ductus Venosus Anatomic descriptions of abnormal termination of umbilical veins with absence of ductus venosus are rare anxiety 2 days after drinking order tofranil american express. Usually, the absence of the ductus venosus and abnormal termination of the umbilical veins do not produce symptoms; however, two cases of intrauterine obstruction of the umbilical vein flow and three patients who required operation for postnatal intestinal obstructions secondary to the anomalous termination of the umbilical veins have been reported (76,77,78,79,80). The major clinical importance of these anomalies is the need to recognize them during prenatal and postnatal diagnostic studies and at the time of cannulation or catheterization of the umbilical vein in sick neonates. Anatomy Lucas and Krabill (52) reported autopsy findings of four specimens in the Jesse Edwards Registry of Cardiovascular Pathology P. In four patients, the persisting umbilical vein could not be identified as either right or left. Clinical Manifestations Of the 23 collected cases, 10 patients were male, 10 were female, and in 3 the gender was unknown or ambiguous. Only four patients had clinical evidence of abnormal physiology as a result of the abnormal termination of the umbilical vein; one had anatomic evidence of severe intrauterine obstruction of umbilical vein flow (77). Intestinal obstruction requiring surgical intervention was present as a result of the anomalous termination of the umbilical vein in three patients (78,79,80). The number of umbilical arteries was identified in 16 patients; one umbilical artery was present in nine patients, two in the remainder. Diagnostic Features Definitive anatomic diagnosis was accomplished by the following methods: catheterization of the umbilical vein, dye injection plus local surgical dissection of the umbilical vein, cardiac catheterization, cardiac catheterization plus angiography, prenatal echocardiography, postnatal echocardiography, and at the time of operation for intestinal obstruction. The major clinical importance of these cases is the potential for confusion and misinterpretation during catheterization of the umbilical vein in the neonate or abnormal course of the catheter in newborns undergoing cardiac catheterization by way of the umbilical vein; however, the increasing use of fetal echocardiography as well as echocardiography early in the postnatal period makes the noninvasive recognition of these anomalies of termination of the umbilical veins possible. These intrahepatic portosystemic shunts are due to abnormal persistence of elements of the omphalomesenteric system. Clinical Manifestations Three of the 10 cases reported (82) resulted in portal-systemic encephalopathy. If ligation of the ductus venosus is contemplated, one should establish the integrity of the portal system. If it is not intact, ligation could lead to mesenteric venous congestion and ultimately bowel ischemia. Persistent Valves of the Sinus Venosus this section is based on the excellent description of Lucas and Krabill (52). Minor abnormal persistence of the valves of the sinus venosus results in larger-than-usual eustachian and thebesian valves and in Chiari networks. The latter are fine, filamentous structures that may represent persistence of either the right or left valves. Usually, Chiari networks are persistent right valves and extend from the crista terminalis to eustachian or thebesian valves. Recent developments in noninvasive imaging have resulted in clinical recognition of numerous instances of persistence of the right valve of the sinus venosus.
Buy tofranil 25 mg on-line
Closure of the fenestration in the extracardiac Fontan with the Amplatzer duct occluder device anxiety symptoms upper back pain order cheap tofranil line. Preoperative transcatheter closure of congenital muscular ventricular septal defects. Primary transcatheter umbrella closure of perimembranous ventricular septal defect. Transcatheter closure of multiple muscular ventricular septal defects using Gianturco coils. Multicenter experience with perventricular device closure of muscular ventricular septal defects. Device closure of muscular ventricular septal defects using the Amplatzer muscular ventricular septal defect occluder: immediate and mid-term results of a U. Transcatheter closure of large patent ductus arteriosus (> or = 4 mm) with multiple Gianturco coils: immediate and mid-term results. Long-term outcome of transcatheter coil closure of small to large patent ductus arteriosus. Risk of coronary artery compression among patients referred for transcatheter pulmonary valve implantation: a multicenter experience. Percutaneous tricuspid valve replacement in congenital and acquired heart disease. Percutaneous replacement of pulmonary valve using the Edwards-Cribier percutaneous heart valve: first report in a human patient. Stenting of the ductus arteriosus and banding of the pulmonary arteries: basis for various surgical strategies in newborns with multiple left heart obstructive lesions. Surgical preconditioning and completion of total cavopulmonary connection by interventional cardiac catheterisation: a new concept. Intraoperative device closure of perimembranous ventricular septal defects without cardiopulmonary bypass: preliminary results with the perventricular technique. Completion angiography after cardiac surgery for congenital heart disease: complementing the intraoperative imaging modalities. Intraoperative assessment after pediatric cardiac surgical repair: initial experience with C-arm angiography. Pickoff In this chapter, current concepts regarding the formation of the cardiac conduction system, along with developmental aspects of cardiac electrophysiology, are summarized.
Aschnu, 22 years: Infection of the dorsal aspects of feet and hands is considered to be tinea corporis. The coil occlusion device usually is delivered into a vessel with a discrete distal narrowing, where it will fix in place and not migrate further through the vessel.
Dennis, 54 years: Patent Ductus Arteriosus Classic studies by Gittenberger-de Groot have described the sequence of events that occur in the infants that lead to functional and anatomic closure of the ductus arteriosus (3). This type of cooperation with inclusion of the adjunct procedures of the cardiologist in the staging of the surgery will contribute to a better outcome for many patients with extremely complex lesions.
Quadir, 35 years: They are not the ideal diagnostic test in children less than 4 years old, as sensitivity is quite low. Patterns and values considered abnormal in adults are often found in normal children.
Kan, 39 years: If dissolved oxygen is not taken into account in flow calculations, the amount of flow/shunt may be overestimated. This information may be helpful in evaluating right ventricular size and function in the following settings: a) Postoperative tetralogy of Fallot (to guide timing of pulmonary valve replacement) or b) systemic right ventricle.
Bozep, 47 years: Beneath this commissure is either a distinct medial papillary muscle or, more commonly, multiple direct chordal insertions along the septum. In very small patients, stents should be avoided unless the stent utilized has the capacity to later be enlarged to adult diameter.
Steve, 64 years: Peripheral pulmonary artery stenosis is often multifocal and associated with syndromes like Williams�Beuren, Alagille, Ehlers�Danlos, and Takayasu arteritis. Secondary attack rates for unvaccinated contacts are estimated to range from 37% to 88%.
Candela, 46 years: Left: Normal heart pathologic specimen cut in short axis at the base demonstrating where the atrioventricular junction has a figure-of-eight configuration. A 1-day regimen of valacyclovir (2 g twice daily for 1 day) decreased the mean duration of cold sore episodes by 1 day when compared with placebo, if started in the prodrome period.
Emet, 24 years: In ventricular D-loop, the palm of the right hand is placed over the septum with the thumb in the tricuspid valve and the fingers in the right ventricular outflow tract. While the physicists prefer the former, most manufacturers use the latter definition.
Kulak, 27 years: In 1905, William Osler, described the term "parchment heart," but Henry Uhl reported the first case in 1952 (141). The segment of the dorsal aortae between the third and fourth pair of aortic arches involutes, disconnecting the distal third aortic arches from the dorsal aortae.
Jaroll, 63 years: Use of rapid-deployment extracorporeal membrane oxygenation for the resuscitation of pediatric patients with heart disease after cardiac arrest. Electrophysiological study of young patients with exercise related paroxysms of palpitation: role of atropine and isoprenaline for initiation of supraventricular tachycardia.
Ur-Gosh, 50 years: The syndrome is characterized by maldevelopment of the third and fourth pharyngeal pouch, with a broad array of symptoms including aortic arch anomalies (particularly those related to the fourth aortic arch), conotruncal abnormalities, abnormal facies, cleft palate, parathyroid hypoplasia with secondary hypocalcemia, and thymic hypoplasia with secondary cellular immunodeficiency (9). Monkeypox is a zoonotic infection endemic in Africa, but it has recently appeared in the Western Hemisphere.
Sugut, 43 years: During the procedure, the position of sheaths and guide wires should be documented and communicated to the interventionalist. Difficulties in Distinguishing Normal from Abnormal Diastolic Function in Children Throughout this section we have discussed differences between adults and children and difficulties, especially in children, in interpreting diastolic function.
Mitch, 42 years: Various methods of timing have been used and include automated bolus tracking, the use of a precontrast test bolus, and empiric methods (31). When the pulmonary vascular resistance decreases in the newborn period, retrograde flow in the ipsilateral vertebral artery is directed mainly into the arterial duct toward the pulmonary vascular bed, because the pulmonary resistance is less than that of the arm.
Hengley, 45 years: This boosts the radiation dose three to four times compared to a nongated examination. Those patients with a right aortic arch with mirror-imaged branching and no associated intracardiac disease frequently have stenosis or atresia of the left pulmonary artery (15).
Mason, 36 years: In general, if the patient has a right aortic arch with mirror-imaged branching, there is a very high likelihood of associated intracardiac disease, while if the patient has a right aortic arch with abnormal arch branching, the incidence of associated intracardiac disease is low. They have demonstrated good in vitro and in vivo activity against Nocardia asteroides complex, good in vitro sensitivity against A.
Jensgar, 53 years: In most of the cases reported in the literature, medial hypertrophy of the pulmonary arterioles is present. A twin study has provided compelling evidence that both genetic and environmental factors are important in determining disease susceptibility and expression.
Basir, 33 years: The second stage, done at the time of the bidirectional cavopulmonary anastomosis at 3 to 6 months of age, includes the aortic reconstruction. Excessive pulmonary blood flow is heralded by high oxygen saturations even on low FiO2, and low diastolic blood pressures; coronary ischemia and cardiovascular collapse is possible.
Kelvin, 37 years: Subcostal two-dimensional echocardiographic identification of right superior vena cava connecting to left atrium. In addition, such a high-volume, high-pressure shunt over time can lead to irreversible pulmonary vascular disease (Eisenmenger syndrome).
Folleck, 57 years: Fetal infection with B19 may result in either an unaffected fetus or spontaneous abortion (especially in the first half of pregnancy), hydrops fetalis in the second half of pregnancy, congenital anemia, and even late fetal death. Transesophageal echocardiographic guidance of transcatheter ventricular septal defect closure.
10 of 10 - Review by D. Lares
Votes: 110 votes
Total customer reviews: 110