Olmesartan
Olmesartan dosages: 40 mg, 20 mg, 10 mg
Olmesartan packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Purchase olmesartan 10 mg free shipping
Persistent lymphopenia and slow T-cell reconstitution is primarily responsible for vulnerability to infections during this period can blood pressure medication kill you order olmesartan uk. This combination of poor T-cell function and need for additional immune suppression predisposes children to an increased risk of latent viral reactivations, poor outcomes from typically selflimiting primary viral infections, and invasive mold disease. Additionally, this period is an important window of risk for Pneumocystis jirovecii pneumonia; therefore all patients continue prophylaxis through this period and often until T-cell reconstitution. Bacteremia, sinusitis, upper respiratory tract infections, pneumonia, and meningitis are not infrequently caused by encapsulated bacteria (Streptococcus pneumoniae, Haemophilus influenzae, Neisseria meningitidis) during this period. In addition to encapsulated organisms, bacteremia during this period may also result from Staphylococcus species or gram-negative bacteria. Although the peak of reactivation of latent viruses is in the early post-engraftment period, the risk persists through this late phase. For Epstein-Barr virus, reactivation can lead to the development of posttransplant lymphoproliferative disease, which typically presents between 3 and 5 months after transplant. Other atypical late post-engraftment infections may be due to Nocardia species, Listeria species, Cryptococcus species, and nontuberculous mycobacteria. For each method, there are two approaches to guide initiation or duration of prophylaxis: a uniform time at risk approach or an individualized approach that takes into account ongoing immunosuppression and immune reconstitution. With the uniform time-at-risk approach, antimicrobial prophylaxis is continued until a designated time period elapses. Much of the data on the effectiveness for prophylaxis have evolved from trials designed with this simpler standardized time-at-risk approach. Although it has the advantage of consistency and ease of use, this approach likely results in overtreatment of some patients and undertreatment of others. This system is much more cumbersome and has less evidence to support its use; however, it should theoretically result in earlier discontinuation of prophylaxis for some patients with adequate immune reconstitution and appropriately prolong prophylaxis for patients with immune defects that persist beyond an estimated risk period duration from transplantation. Whether a center uses the fixed time-at-risk approach or a more individualized approach will depend on the infrastructure of the transplant center and its ability to consistently apply a more nuanced approach to prophylaxis. The delayed use of live-attenuated vaccines is based on concerns about transmission of vaccine-mediated disease and limited clinical data on safety or immunogenicity of earlier vaccination. This occurs in several phases, resulting in recovery of specific components of the immune system at distinct time points (Table 2. Innate Immune Recovery After Transplantation the innate immune system can be divided into nonhematopoietic and hematopoietic compartments. The nonhematopoietic compartment includes physical barriers, such as the skin and mucosal surfaces, which can be damaged during transplantation by the pretransplant conditioning regimen. The skin and mucosal barriers can also be compromised by the presence of foreign material, such as a central venous catheter or a gastrostomy tube, for prolonged periods after transplantation. After myeloablative conditioning, patients undergo an aplastic phase, which is identified by severe neutropenia, anemia, and thrombocytopenia. The first laboratory sign of hematologic recovery is typically neutrophil recovery. Engraftment, classically defined as absolute neutrophil count greater than 500/mL, is typically achieved between 10 and 42 days and transplant, depending on the stem cell source (see Table 2.
Diseases
- Donnai Barrow syndrome
- Progressive supranuclear palsy atypical
- Fanconi ichthyosis dysmorphism
- Ciliary discoordination, due to random ciliary orientation
- African trypanosomiasis
- Autoimmune hepatitis
- Potter syndrome dominant type
- Dissociative identity disorder
Olmesartan 10 mg order amex
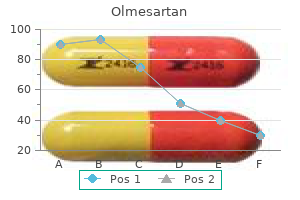
In terms of their neuro-computational properties blood pressure vs blood sugar buy generic olmesartan 10 mg online, Type I neurons are integrators (see Section 8. It is labeled as a resonator because the stimulus for such a neuron is most effective if its frequency is the same as that of the subthreshold oscillations. A neuron whose membrane voltage following a perturbation does not oscillate as it approaches the resting value is an integrator, since successive stimuli are more effective in causing fring because of a cumulative, or integrating, effect. The membrane voltage of an integrator is shown returning smoothly, without oscillations, to the steady membrane voltage level, which may or may not be the resting level. A second pulse at t1 will take the membrane voltage beyond threshold and will cause fring, whereas a pulse at t2 will not. The effect is similar to that of temporal and spatial summation discussed in Section 7. Neuronal Firing Patterns and Models 279 In (b) a brief, subthreshold pulse is also applied at t0. However, the membrane voltage of a resonator is shown returning to the steady level with damped oscillations. The stimulus is most effective in fring a resonator if its frequency is the same as, or close to , that of the subthreshold oscillations and the timing of the stimulus is such that the pulses occur at or near the maxima of the oscillations. Increasing or decreasing the stimulus frequency outside the optimum range makes the stimulus less effective. In contrast, as the frequency of the stimulus to an integrator is increased, the stimulus becomes more effective in fring, and fring occurs sooner. A high-frequency burst of pulses applied to a resonator may not cause fring at all if the pulses occur near the minimum of the subthreshold oscillations. If the pulse at t1 occurs at an oscillation minimum, the oscillations that it produces will tend to cancel out the oscillations due to the pulse at t0 in which case a pulse at t2 may not cause fring. Effectively, the pulse at t1 will thus inhibit fring due to the pulse at t2, although the pulse at t1 is depolarizing. Thus, if neuron A excites two resonators B and C having different frequencies of subthreshold oscillations, then neuron B, but not C, can be fred when neuron A fres at a frequency equal to that of the subthreshold oscillations of neuron B. In integrators, fring is determined by excitatory and inhibitory synaptic inputs at any instant. Evidently, a larger repertoire of responses is possible with resonators compared to integrators. The frequency of subthreshold oscillations in resonators ranges between a few Hz and about 200 Hz, the amplitude being generally a few millivolts at the resting voltage. However, both the amplitude and the frequency of the oscillations increase with background depolarization, the amplitude increasing to more than 10 mV peak-to-peak in some cases. Moreover, background synaptic activity continuously perturbs the membrane voltage and can make the subthreshold oscillations effectively continuous.
10 mg olmesartan visa
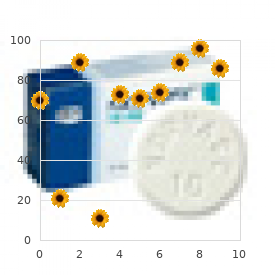
The ultra-rapid freezing allows temporal resolution of cellular events heart attack jim jones discount olmesartan online master card, that is, examining these events at various stages of their evolvement. The amplitude of the mepps varies in accordance with a unimodal, approximately normal distribution around a mean value that is generally between 0. The variance in the distribution is due to variation in the number of neurotransmitter molecules per vesicle, in the number of neurotransmitter molecules that bind to receptors, and in the kinetics of channel opening after the binding of a neurotransmitter. We will frst derive the probability density function for the interval between successive releases. A basic assumption is that the release of a vesicle does not affect the release of other vesicles, that is, the release of a vesicle does not depend on the past history of vesicle release. Assuming that a vesicle is released at t = 0 and that the interval t until the next release is divided into m increments of Dt, that is, mDt = t, then p(t + Dt), the probability of the next vesicle being 158 Neuromuscular Fundamentals released during the increment Dt following the end of the interval t, is the product of its not being released during any of the m increments of t and the probability of its being released during the increment Dt at the end of t, that is, p(t + Dt) = (1 - r Dt)m r Dt (5. From the defnition of the probability density function, f1(t)dt is the probability that the interval X between successive releases will have a value between t and t + dt. This means that in a large number N of intervals between releases, the number of occurrences dn of any interval between t and t + dt is: dn = Nf1(t)dt = Nre - rt dt (5. The number of intervals n with a duration less than or equal to t is the integral of dn in Equation 5. Experimental recordings of intervals between successive mepps show an exponential distribution for short intervals and a power-law distribution over intervals of 1 s or more. The exponential distribution refects a random, memoryless process, as assumed in the preceding discussion. The power law is due to a nonrandom process, such as that of recycling and repackaging of synaptic vesicles. The probability density for the time to release the second, third, or kth vesicle, following the release of a vesicle at t = 0, will be determined next. To have a second release at time t, there must be a frst release at an intermediate time u < t. Hence this product is the infnitesimal df2(u)dt, where f2(t) is the probability density for the time to release the second vesicle. For k = 1, f k(t) = f1(t), that is, the probability density function for a single release is the same as the probability density function of the interval between successive releases, which is an exponential distribution (Equation 5. At t = 0, f1(t) = r, in accordance with the interpretation that f1(t)Dt is the probability of a single release between t = 0 and t = Dt, which is rDt. The probability of more than one release in the time interval between t = 0 and t = Dt is small and decreases with increasing k.
Olmesartan 20 mg order free shipping
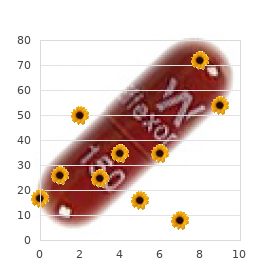
Transitional cell carcinoma of the ovary is related to high-grade serous carcinoma and is distinct from malignant Brenner tumor heart attack aspirin purchase olmesartan on line amex. Transitional cell carcinoma of the ovary: a morphologic study of 100 cases with emphasis on differential diagnosis. Ovarian Brenner tumour: a morphologic and immunohistochemical analysis suggesting an origin from fallopian tube epithelium. Endometrial and ovarian carcinomas with undifferentiated components: clinically aggressive and frequently underrecognized neoplasms. Carcinosarcoma of the ovary, fallopian tube, and peritoneum: prognostic factors and treatment modalities. Endocervical-like mucinous borderline tumors of the ovary: a clinicopathologic analysis of 31 cases. Mucinous tumors of the ovary: a clinicopathologic analysis of 75 borderline tumors (of intestinal type) and carcinomas. Primary ovarian mucinous carcinoma of intestinal type: significance of pattern of invasion and immunohistochemical expression profile in a series of 31 cases. A clinicopathologic analysis of atypical proliferative (borderline) tumors and well-differentiated endometrioid adenocarcinomas of the ovary. Identifying Lynch syndrome in patients with ovarian carcinoma: the significance of tumor subtype. High frequency of beta-catenin mutations in borderline endometrioid tumours of the ovary. Sertoliform endometrioid carcinomas of the ovary: a clinicopathologic and immunohistochemical study of 13 cases. Molecular-based classification algorithm for endometrial carcinoma categorizes ovarian endometrioid carcinoma into prognostically significant groups. Endometrioid neoplasms with clear cells: a report of 21 cases in which the alteration is not of typical secretory type. Nucci this category includes a diverse group of neoplasms believed to derive from the hormone-producing ovarian cortical stroma. If present, sex cord elements (granulosa cells) must be minor (<10% of the tumor). Most fibromas are incidental findings removed at the time of surgery for an unrelated condition; however, abdominal pain is the presenting symptom in approximately 40% of cases. They are uncommon in women <30 years, except for patients with Gorlin syndrome (nevoid basal cell Conventional fibromas are typically unilateral (90%) and may range from microscopic to >20 cm (average 6 cm). Edema and pseudocyst formation are frequent; calcification is seen in up to 10% of tumors.
Yougurt (Yogurt). Olmesartan.
- High cholesterol levels.
- Asthma.
- Are there safety concerns?
- How does Yogurt work?
- Diarrhea in malnourished infants and children.
- What other names is Yogurt known by?
- Dosing considerations for Yogurt.
- Preventing vaginal yeast infections.
- Diarrhea in children.
- Treating a bacterial infection that can cause stomach ulcers (Helicobacter pylori), when used in combination with other medicines.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96805
Best 40 mg olmesartan
Given their benign outcome heart attack get me going cheap 40 mg olmesartan with amex, conservative surgery is appropriate in the initial management of these lesions, especially in young, reproductive-aged women. Unilateral salpingo-oophorectomy, with careful examination for extraovarian disease, is sufficient treatment. Mucinous borderline tumors with stromal microinvasion are probably not associated with an increased risk of recurrence, but relatively few cases have been reported. Occasional (<5%) mucinous borderline tumors with intraepithelial carcinoma have recurred as high-grade carcinoma within 5 years of initial diagnosis. These tumors have been associated with a rapidly progressive course, frequently with distant metastases. Patients are either asymptomatic or present with abdominal enlargement or pain and, less frequently, with changes 614 in bowel or bladder function. Surface ovarian involvement is not identifiable in most cases, although larger tumors may exhibit rupture and/ or adhesions. Typically, primary mucinous carcinoma demonstrates a continuum of architectural and cytologic atypia that includes borderline and frankly carcinomatous areas. Invasive carcinoma can be diagnosed based on two different patterns of invasion, which may coexist in a single tumor. The presence of stromal invasion, whether of destructive or confluent type, must exceed 5 mm in linear extent to warrant classification as carcinoma; otherwise, a diagnosis of microinvasion or microinvasive carcinoma is rendered. Recognizable mucinous epithelium may give way to a frankly anaplastic carcinoma, especially in tumors showing destructive stromal invasion. The grading of mucinous carcinomas is not uniform among practices, as there is no universally accepted system. It is more important to note if the tumor contains infiltrative invasion, intraepithelial carcinoma, or microinvasive carcinoma as defined earlier. Complex mass shows cysts filled with mucoid material, admixed with solid soft areas with a similarly mucoid cut surface. Staining for p16 is negative or patchy, unless the tumor is uniformly high grade or harbors anaplastic carcinoma. A confluent cribriform architecture diagnostic of carcinoma (right) coexists with foci of mucinous borderline tumor (left) (A). Most tumors show an expansile pattern of invasion, in which glands are crowded and confluent (back to back) with minimal intervening stroma (B). As an important caveat, a mucinous tumor arising in a teratoma will show an immunophenotype identical to primary lower gastrointestinal tumors.
20 mg olmesartan order with mastercard
Herpesviruses arteria sacralis mediana olmesartan 10 mg buy mastercard, which possess a unique ability in their life cycle to establish latent infection, are especially significant within these patient populations because of their capacity to reactivate in the setting of immunosuppression. Symptoms that occur with viral replication are primarily associated with the immune response to the infection rather than direct viral destruction; therefore symptoms may be blunted in immunocompromised hosts with an ineffective immune response. This primary immune response is sufficiently restricted, however, to allow the virus to establish latency rather than be eradicated. Humoral immune responses mediated by B cells are also needed for immune memory, but viral reactivation can occur despite adequate antibody responses in infected individuals. Recurrent infection may result from reactivation of latent virus (endogenous) or reinfection (exogenous). Cytomegalovirus risk, prevention, and management in pediatric solid organ transplantation. Prophylaxis occurs when antiviral therapy is provided to all (universal) or at-risk (targeted) patients for a predetermined period of time after transplantation. A mixed model of short-term prophylaxis followed by surveillance at scheduled intervals, currently referred to as "surveillance after prophylaxis", can also be used. These two factors have primarily driven recommendations around the choice of preventative strategy and duration of intervention. Overall, either prophylaxis for a predetermined duration, usually 3 to 12 months depending or organ transplanted, or surveillance after prophylaxis is recommended. As assay results can be affected by sample type (serum, plasma, or whole blood), assay primers, and extraction methods, consistency in these parameters should be paramount and appropriate comparisons performed with any modification of testing methods. Surveillance, monitoring for progression of disease, monitoring of response to treatment. Detection of viral shedding; many centers are using this test in place of shell vial culture for screening of infants. More difficult to interpret treatment response, no longer widely available; not reliable in neutropenic patients. Generally, intravenous therapy is suggested for patients with severe disease or those who have significant concerns with absorption of oral agents. As noted earlier, concerns exist for marrow suppression with ganciclovir/valganciclovir before engraftment; in these circumstances, alternate agents, such as foscarnet and less commonly cidofovir, have been used. For patients receiving ganciclovir therapy, options include increased doses of ganciclovir and addition or transition to foscarnet while genetic resistance test results are pending. Results of resistance testing and specific clinical scenarios including risks for antiviral toxicity should be considered in the development of individualized antiviral treatment plans. Significant T-cell depletion, high viral loads, and suboptimal antiviral concentrations may all contribute to development of resistance. In children, dose optimization with weight gain and changes in renal function is critical to ensuring adequate antiviral drug levels and avoiding resistance. The most practical assessment of antiviral resistance is currently a genotypic assay to sequence the genes in which antiviral resistance mutations are known to occur.
40 mg olmesartan order free shipping
Invasive fungal infections in pediatric heart transplant recipients: incidence arrhythmia technology institute south carolina cheap olmesartan line, risk factors, and outcomes. The 2015 International Society for Heart and Lung Transplantation Guidelines for the management of fungal infections in mechanical circulatory support and cardiothoracic organ transplant recipients: executive summary. Invasive fungal infections in pediatric oncology patients: 11-year experience at a single institution. Risk factors for infection-related outcomes during induction therapy for childhood acute lymphoblastic leukemia. Risk factors and predictors for candidemia in pediatric intensive care unit patients: implications for prevention. Failure to validate a multivariable clinical prediction model to identify pediatric intensive care unit patients at high risk for candidemia. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Antifungal prophylaxis in cancer patients after chemotherapy or hematopoietic stem-cell transplantation: systematic review and meta-analysis. Guideline for primary antifungal prophylaxis for pediatric patients with cancer or hematopoietic stem cell transplant recipients. Randomized, double-blind trial of fluconazole versus voriconazole for prevention of invasive fungal infection after allogeneic hematopoietic cell transplantation. Antifungal agents for preventing fungal infections in solid organ transplant recipients. Randomized, double-blind trial of anidulafungin versus fluconazole for prophylaxis of invasive fungal infections in high-risk liver transplant recipients. A randomized, prospective, doubleblinded evaluation of selective bowel decontamination in liver transplantation. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the infectious diseases society of america. Finding the "missing 50%" of invasive candidiasis: how nonculture diagnostics will improve understanding of disease spectrum and transform patient care. T2 magnetic resonance assay for the rapid diagnosis of candidemia in whole blood: a clinical trial. T2Candida provides rapid and accurate species identification in pediatric cases of candidemia. Diagnostic performance of 1n3-beta-d-glucan in neonatal and pediatric patients with Candidemia. Quantification of 1,3-beta-D-glucan levels in children: preliminary data for diagnostic use of the beta-glucan assay in a pediatric setting. Performance of 1,3-beta-D-glucan for diagnosing invasive fungal diseases in children.

Order olmesartan canada
Decidual change involving the submucosal stroma and mildly expanding the plica (A) arrhythmia list discount olmesartan 40 mg without a prescription. Ectopic decidua in the tubal serosa (B, upper right; high magnification in inset). Tubal torsion leads to extensive hemorrhagic necrosis, more pronounced in the submucosa (B). Temporary (self-limited) torsion is usually subclinical and manifests with intermittent pelvic pain. Torsion is more likely to occur after tubal enlargement secondary to hydrosalpinx, pyosalpinx, abscess, or occlusion. The adnexal vessels (particularly the veins) are significantly dilated and frequently contain recent or organizing thrombi. Even if the tissue is massively infarcted, a neoplastic proliferation will be identified microscopically in most cases. Extensive hemorrhage can also be due to trauma, endometriosis, or ectopic gestation. Unlike torsion, in these scenarios the adnexal vessels are not congested or occluded, and the tubal wall is viable. Macroscopic changes vary depending on the duration and the severity of blood flow obstruction. In massively infarcted tubo-ovarian specimens, it may be difficult to identify the fallopian tube and separate it from the engorged and hemorrhagic tubo-ovarian soft tissue. Complete tubal torsion with secondary infarction requires urgent surgical excision of the tube with or without the ovary. Complications include auto-amputation of the adnexa, rupture with hemoperitoneum, and superimposed infection. Race and Age Distribution n Predominantly seen in reproductive-age women Clinical Features n Acute and severe low abdominal pain n Urinary frequency Prognosis and Treatment n Suspension of adnexa in cases of intermittent torsion n Emergency surgery (salpingectomy or salpingo-oophorectomy) if complete torsion complicated with infarction fallopian tube caused by diverticula of tubal epithelium into the muscular wall. The pathogenesis and etiology of this disease remain unclear; some authors have postulated a congenital origin, whereas others favor an acquired process, possibly postinflammatory. The lesion is otherwise asymptomatic and discovered incidentally during work-up for infertility or ectopic gestation. Other techniques include laparoscopic chromopertubation, salpingoscopy, and transvaginal hydrolaparoscopy (the latter allows visualization of the tubal mucosa). Two-thirds of the cases occur in the right tube and one-third in the left; only 4% are bilateral. On cut section, visibly dilated diverticular structures can be observed within the wall. On high-power examination, the glandular structures are lined by benign tubal epithelium, and connection of the intramural epithelial diverticuli to the mucosa can be sometimes appreciated. Follicular salpingitis produces small glandular spaces in the submucosa, separated by lymphoplasmacytic inflammatory infiltrates and reactive fibroconnective tissue; however, there is no smooth muscle in between glands.
Discount olmesartan online visa
It is more potent than cidofovir against adenoviruses based on the inhibitory concentration of 50% arrhythmia upon waking purchase olmesartan 20 mg visa. Treatment failure (progression to probable or definitive adenovirus disease or increasing adenoviremia) was the primary endpoint. Although the proportion of subjects receiving twice-weekly brincidofovir encountered less treatment failures (21%) compared with the once-weekly brincidofovir group (38%) and placebo (33%), results were not statistically significant. They observed improved virologic response (1 log reduction in 2 weeks) in adenoviremia episodes treated with brincidofovir (83%) compared with cidofovir (83% vs. Virologic response correlated with survival advantage, which could not be explained by immune recovery alone. Additionally, it is currently available only as an enteral formulation, which can be a major barrier to administration for a patient population with frequent gastrointestinal complications. For adenovirus disease some have suggested continuing therapy until complete resolution of the signs and symptoms of disease and documentation of one to three negative adenovirus samples taken 1 week apart from the sites that were originally positive. Ribavirin, a nucleoside analog of guanosine that inhibits the viral polymerase, has antiviral activity limited to species C adenoviruses (serotypes 1, 2, 5, and 6). Treatment with ribavirin was not associated with a significant decrease in the adenovirus viral loads,3,5 Brincidofovir. Ganciclovir has limited activity against adenovirus because it requires phosphorylation by an enzyme called thymidine kinase to convert the agent from a prodrug to its active form that would subsequently inhibit viral replication. Adenoviruses lack thymidine kinase and human kinases are not efficient at phosphorylating ganciclovir to its active state. Nitazoxanide, a thiazolide and its active metabolite tizoxanide, has a low toxicity profile and may have antiviral activity by targeting cellular pathways involved in the syntheses of viral proteins. Intravenous immunoglobulins have been administered in the setting of adenovirus disease, especially for severe cases, with mixed results. Immunotherapy Immunotherapy for invasive adenovirus infection is a promising therapeutic strategy but is not widely available. Acquired hypogammaglobulinemia (immunoglobulin G levels,350 mg/dL) has e1 Abstract: Adenoviruses can complicate the peritransplant course of pediatric solid organ and hematopoietic stem cell transplant recipients. Distinguishing adenovirus infection and disease is an important aspect of clinical management. This article outlines the epidemiology, risk factors, clinical manifestations, diagnosis and management of adenovirus disease in these populations. Adenovirus infection in paediatric stem cell transplant recipients: increased risk in young children with a delayed immune recovery. Management of adenovirus infection in patients after haematopoietic stem cell transplantation: state-ofthe-art and real-life current approach: a position statement on behalf of the Infectious Diseases Working Party of the European Society of Blood and Marrow Transplantation. Prospective assessment of adenovirus infection in pediatric kidney transplant recipients.
Thordir, 39 years: The tight interlocking is necessary to prevent leakage of ions between the channel and the extracellular space. In patients with neutropenia, examination findings, such as chorioretinal lesions, may be present only after neutrophil recovery.
Sanford, 65 years: Larger observational studies incorporating methods to control for confounding, including "natural experiment" analysis based on era of treatment, or propensity score adjustment, have conversely not shown a benefit to combination therapy. The motor association areas are thus able to plan a movement, initiated internally or in response to some external cue, from its starting point to its destination, based on the position of the body in space, on the locations of targets and surrounding objects, and on past experience, motivation, and emotional state.
Quadir, 44 years: Spinocerebellum, comprising the vermis and pars intermedia, and which appears later in phylogeny. Ftw is only a fraction of F0 because of the viscoelastic property of muscle, as will be explained later.
Hernando, 45 years: In both running and walking, movement of the arms helps propel the body forward and enhances body stability. In practice, p is small under conditions of low Ca2+ or high Mg2+, in which case the Poisson distribution applies.
Killian, 63 years: Deaths occur disproportionately among individuals with chronic and/ or immunocompromising conditions, such as transplantation and/ or chemotherapy. Differentiation of ovarian mucinous carcinoma and metastatic colorectal adenocarcinoma by immunostaining with beta-catenin.
Lares, 62 years: It follows that d(nN)/dt, the rate at which the number of gates per unit area in the o position is increasing with time, is equal to n(1 � n)N, the rate at which gates are moving from the c position to the o position, minus nnN, the rate at which gates are moving from the o position to the c position. The lack of statistical significance may have been due to early trial termination.
Bram, 64 years: This peak region extends to point c, with further shortening, when the edges of the thin flaments reach the M line. Some of the axons end, or have collaterals that end, in the motor nuclei of the midbrain, pons, and medulla, whose pathways will be discussed later.
Stejnar, 26 years: Changing epidemiology of infections in patients with neutropenia and cancer: emphasis on gram-positive and resistant bacteria. It is especially important that pediatric transplant candidates receive an infectious disease review that is family-centered and considers occupational and recreational exposures not only for the transplant candidate but also for all other household contacts.
Jaroll, 56 years: Volatile anesthetics interfere with the myocardial calcium regulation and have inhibitory effects additional to those of nifedipine. Mitochondria and glycogen granules are found in the sarcoplasmic space between the myofbrils.
Peer, 47 years: Not surprisingly, the active responses of the soma and dendrites seem to be tailored to the functions of the particular type of neuron. Despite the movement of Cl�, side o must remain positive with respect to side i in order to maintain the required electric potential gradients for the three ions.
8 of 10 - Review by L. Fedor
Votes: 129 votes
Total customer reviews: 129