Motilium
Motilium dosages: 10 mg
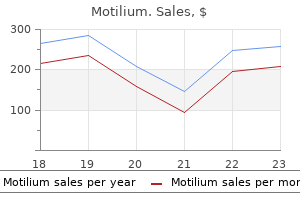
Motilium packs: 90 pills, 180 pills, 270 pills, 360 pills

Buy discount motilium 10 mg line
Results of microsurgical treatment for intramedullary spinal cord ependymomas: analysis of 36 cases chronic gastritis weight loss cheap motilium. Long term outcome with post-operative radiation therapy for spinal canal ependymoma. Tumor control after surgery for spinal myxopapillary ependymomas: distinct outcomes in adults versus children: a systematic review. Proton therapy for spinal ependymomas: planning, acute toxicities, and preliminary outcomes. Prognostic factors for local control and survival after radiotherapy of metastatic spinal cord compression. A score predicting posttreatment ambulatory status in patients irradiated for metastatic spinal cord compression. Final results of a prospective study of the prognostic value of the time to develop motor deficits before irradiation in metastatic spinal cord compression. Initial bolus of conventional versus high-dose dexamethasone in metastatic spinal cord compression. Predictive value of seven preoperative prognostic scoring systems for spinal metastases. Preliminary results of spinal cord compression recurrence evaluation (score-1) study comparing short-course versus long-course radiotherapy for local control of malignant epidural spinal cord compression. Evaluation of five radiation schedules and prognostic factors for metastatic spinal cord compression. The first score predicting overall survival in patients with metastatic spinal cord compression. Recursive partitioning analysis index is predictive for overall survival in patients undergoing 75. Safety and efficacy of stereotactic body radiotherapy as primary treatment for vertebral metastases: a multi-institutional analysis. Long-term safety and efficacy of fractionated stereotactic body radiation therapy for spinal metastases. Outcomes for spine stereotactic body radiation therapy and an analysis of predictors of local recurrence. Retrospective long-term follow-up analysis in 21 patients with chordomas of various sites treated at a single institution. Postoperative spot-scanning proton radiation therapy for chordoma and chondrosarcoma in children and adolescents: initial experience at Paul Scherrer Institute. Particle therapy using carbon ions or protons as a definitive therapy for patients with primary sacral chordoma. Stereotactic fractionated radiotherapy for chordomas and chondrosarcomas of the skull base. Hypofractionated stereotactic radiation therapy for skull base and upper cervical chordoma and chondrosarcoma: preliminary results. Stereotactic body radiotherapy for metastatic and recurrent ewing sarcoma and osteosarcoma.
Cheap motilium 10 mg with visa
Particularly gastritis etiology buy motilium 10 mg cheap, rates of radiation-induced edema are higher for large radioresistant tumors, if relatively high prescription doses are used. In hepatocellular carcinoma, malignant melanoma, choriocarcinoma, and renal cell carcinoma, tumor bleeding rates are reportedly high. The incidence of symptomatic radiation necrosis is usually less than 5%, depending on such factors as target volume, prescription dose, pathology, interval from treatment, dose gradient, conformity, and previous radiation history. Four patients died mainly as a result of adverse events; two had tumor bleeding (1. Each tumor was irradiated with a prescription dose of 13 Gy at the tumor periphery with two-stage Gamma Knife radiosurgery. The tonsillar herniation sign resolved and the neurological symptoms disappeared completely. These lesions were diagnosed as radiation necrosis by methionine positron emission tomography scan. In addition, there were no significant differences in the frequencies of neurological death and neurological function deterioration. The management of recurrent tumors is even more challenging, with no standardized treatment except bevacizumab, a humanized monoclonal antibody against vascular endothelial growth factor. This means an almost 15-cm3 total tumor volume is irradiated with a standard prescription dose of 20 to 22 Gy at the tumor periphery. Furthermore, outcomes of patients with total tumor volumes greater than 15 cm3 are significantly poorer in terms of preventing neurological death and preserving neurological function. Aggressive treatment for brain metastases should also be considered for patients who are expected to be good responders to chemotherapy or molecular targeting agents. Enhancements involving several brain sulci (A), basal cisterns (B), and the ventricular walls (C) are shown (circles). Enhancements of the localized brain sulcus (D), ambient cistern (E), and anterior horn of the lateral ventricle (F) are presented (arrows). Within these limits, 25, 10, or 4 lesions with diameters of 8 mm, 14 mm, or 20 mm, respectively, can be safely irradiated with Gamma Knife radiosurgery using 20- to 22-Gy prescription doses at the tumor periphery, if the tumors are approximately the same size and diffusely located in the brain. The use of bevacizumab may make re-administration of radiotherapy possible in the recurrent setting, given a decreased risk of radiation necrosis as a result of the potent antipermeability of bevacizumab, as demonstrated in a randomized double-blind, placebo-controlled trial. All five of the patients receiving bevacizumab showed a response on the follow-up imaging after two doses, whereas none of the seven patients in the placebo group showed a response. These results seemed superior to those of the landmark randomized trial of bevacizumab alone for recurrent glioblastoma. Ependymoma Ependymoma is a subtype of glioma originating from ependymal cells and more commonly seen in children than in adults. It is more prone to disseminate within the central nervous system than astrocytoma.
10 mg motilium for sale
TumorResponse Long-term follow-up is also needed for evaluation of tumor response in view of the slow growth of a large number of meningiomas gastritis diet 91352 10 mg motilium order visa. In the majority of cases, the morbidity is temporary and rarely disabling, although permanent complications have been reported in 2. Symptomatic peritumoral imaging changes developed in 4% of the patients reported by Kondziolka and colleagues50 at a mean of 8 months and in 9. They are attributable to vasogenic edema with a potential role for vascular endothelial growth factor or radiation injury to the vasculature. Symptoms due to edema may be transient headaches, seizures, and other neurological deficits. Patients with parasagittal,52 parafalcine, and anterior fossa tumor locations are at risk. Patients who present with the first three features or who will receive such doses must be informed about the increased possibility of postoperative edema. The occurrence of a new deficit depends on the dose delivered to the tissue, the length of the nerve segment exposed, and the class of the nerve. We personally reported that failure was observed in two of the three oculomotor deficits that occurred after Gamma Knife radiosurgery of cavernous sinus meningiomas. Vascular occlusion of the intracavernous internal carotid artery has been documented with an incidence of 1% to 2% for cavernous sinus meningiomas. Their etiology is unknown, although they could be due to gliotic scarring or peritumoral edema. The target of radiosurgery is that part of the meningioma whose excision would pose a risk of neurological symptoms. Whether radiosurgery should be delivered routinely in the months following surgery or only in case of tumor regrowth is still debatable. Malignant and atypical meningiomas are clearly more likely to fail to respond to radiosurgery. The therapeutic approach thus differs according to whether the aim of the treatment is to control signs of hormone hypersecretion (for instance, in a secreting microadenoma) or to reduce tumor volume (for instance in a large nonsecreting pituitary adenoma). In most secreting pituitary adenomas, except for prolactinomas, transsphenoidal surgery is the treatment of choice; however, this surgical approach does not always achieve definite remission, and efficacious adjunctive treatment is often needed. Antisecretory drugs are inconsistently effective and are sometimes poorly tolerated, and conventional radiotherapy, although highly effective, induces high rates of panhypopituitarism. In other cases, surgery is contraindicated or impossible, because of cavernous invasion, for instance. Staged radiosurgery has been proposed,66 but data to support this option are not available. Another proposition is to deliberately uncover the whole volume of the tumor and to spare a compartment that either is not supposed to grow or will not put the patient at risk if it does. We personally believe that extension to the paranasal sinuses or to the infratemporal fossa occurs with large meningiomas but does not routinely require treatment.
Generic motilium 10 mg buy on-line
Lack of tocopherol in peripheral nerves of vitamin E-deficient patients with peripheral neuropathy gastritis diet ���������� purchase 10 mg motilium otc. Peripheral neuropathy in chronic occupational inorganic lead exposure: a clinical and electrophysiological study. The basis of the paradoxical disturbance of temperature perception in ciguatera poisoning. Tetrodotoxic poisoning from ingestion of a porcupine fish (Diodon hystrix) in Papua New Guinea: nerve conduction studies. Divalent cation competition with [3H]saxitoxin binding to tetrodotoxin-resistant and -sensitive sodium channels. Critically ill polyneuropathy: electrophysiological studies and differentiation from GuillainBarre syndrome. Interventions for preventing critical illness polyneuropathy and critical illness myopathy. Effects of early treatment with immunoglobulin on critical illness polyneuropathy following multiple organ failure and gram-negative sepsis. Joint Task Force of the European Federation of Neurological Societies/Peripheral Nerve Society. Report of a joint task force of the European Federation of Neurological Societies and the Peripheral Nerve Society. They test large-fiber axons of the motor and proprioception systems, not the small fibers or unmyelinated fibers of the pain, temperature, or autonomic systems. Recordings from near the axons are used to assess sensory nerves, although only the large-fiber axons contribute to the data. Relative to the position of the stimulating electrode, the recording electrode can be placed either orthodromically at a more proximal site (normal direction of propagation) or antidromically at a more distal site. The signal is recorded as the nerve-conducted axon volley passes under the recording electrode. Latency divided by distance yields a conduction velocity (in meters per second, same as millimeters per milliseconds). Latency is the time from stimulation to the beginning of the recorded signal deflection. Measurements are in terms of the latency to response onset, the amplitude of the response, and the conduction velocity. Some distal latency studies use a preset distance with normalized standard limits to determine if a latency is in the normal range. Similar to sensory testing, results are measured by latency, amplitude, and velocity. Regions of severe demyelination completely block conduction so recordings show an absent response. To complicate this simplicity, however, when demyelinating lesions cause conduction block, this can result in decreased amplitude.
Buy generic motilium pills
This condition can manifest as local swelling and stiffness and gastritis vs gerd symptoms motilium 10 mg buy low price, in severe cases, may be associated with erythema and heat. Standing on the affected leg often causes pain, and the patient often has difficulty using the affected leg for support. The distinguishing characteristic of pain originating in the knee is its location on the joint; radicular pain usually begins at the spine and radiates to the anterior aspect of the thigh and knee. Other findings commonly associated with knee disease include instability with associated gait difficulties, knee "locking," erythema, swelling, and inability to extend the knee. MyofascialTriggerPointPain Myofascial trigger point pain is an extremely common cause of persistent pain and can be present throughout the body. Features include deep aching pain in any structure that is referred from focally tender points in taut bands of skeletal muscle. The diagnosis can be established by elicitation of the described pain with palpation using 2 to 4 kg/cm2 of pressure for 10 to 20 seconds over the suspected trigger point. Myofascial pain is frequently found among patients in whom lumbar spine surgery is unsuccessful, and this diagnosis should be identified as a potential cause of pain during the preoperative work-up. This condition might be caused by the presence of an abnormal fibrous band that originates in an elongated C6 or C7 transverse process and ends at the first rib or the pleural cupola. Sensory changes appear to affect predominantly the ulnar nerve, and motor changes predominantly the median nerve. This nerve provides motor fibers to the supraspinatus and infraspinatus muscles as well as conveying sensory information from the glenohumeral and acromioclavicular joints. Compression of this nerve is rare, although it is more prevalent among males and volleyball players. Such compression can result from cysts in the glenohumeral joint or from compression at the suprascapular notch. It manifests as pain in the scapular region that can radiate to the arm and can mimic the symptoms of intrinsic shoulder pathology or cervical radiculopathy. In general, patients with suprascapular nerve compression do not give a history of trauma. This condition can cause weakness during external rotation and abduction of the shoulder as well as atrophy of the infraspinatus muscle, either alone or in combination with atrophy of the supraspinatus muscle. However, diagnostic imaging is often not helpful, particularly when compression occurs at the level of the transverse ligament. Disorders of the Peripheral Nerves Patients with neuropathy can present with weakness, pain, and sensory loss. The presence of these symptoms in individuals with concomitant spondylosis or stenosis can lead to unnecessary surgery. In general, the key to diagnosis is establishing the presence of typical sensory and motor disturbances on history, physical examination, and diagnostic work-up. For further analysis and discussion of each of the entities listed here, please see the peripheral nerve section of this book, Chapters 244 through 258.
Generic motilium 10 mg line
Pain gastritis diet ������� purchase motilium with a visa, fever, and other clinical symptoms may take weeks to improve, and imaging abnormalities may take months. From a treatment perspective, this supports the argument to obtain a biopsy sample before antibiotic therapy is started; knowing the correct antibiotic to use helps physicians manage patients through this difficult period. In the event of disease progression, stopping antibiotic therapy and obtaining a new biopsy sample may be the only way to identify an indolent organism or superinfection. My colleagues and I consider surgery for a patient if after 1 or 2 weeks of bed rest the patient remains unable to be mobilized in a brace. Pain unresponsive to antibiotic therapy may be a sign of instability or resistance to antibiotic therapy. Significant deformity itself is an indication for surgical intervention, which helps speed the healing process by decreasing the infectious burden. Once it has been determined that surgery is indicated, the goals of surgery are complete macroscopic removal of the infected tissues, restoration of the anterior column, and stabilization of the affected levels, with particular attention to anterior column reconstruction. Anterior grafting with anterior instrumentation alone, with posterior instrumentation, with anterior and posterior instrumentation, or through a posterolateral approach with posterior instrumentation through the same incision all yield similar reinfection rates. Of interest is that patients who underwent only decompression for spine infection had similar rates of reoperation and continued infection as did patients who also underwent supplementary instrumentation. In addition, many treatment alternatives are available to the surgical team with regard to approach, graft material, instrumentation, and construct length. It is obvious that there is often more than one way to approach the surgical plan. The following discussions concern a few clinical scenarios and potential treatment options. In 2008, Petracchi and associates22 presented their experience with 11 cases; since then, an additional 12 cases were monitored until documented fusion had occurred. The posterolateral approach is not an option in this region; on the other hand, the anterior approach is a benign, commonly used approach for the experienced surgeon. Another advantage of the anterior approach in the subaxial cervical spine is the ability to effectively immobilize this area externally with a brace or halo vest, if needed. My preference, unless otherwise contraindicated, is to stabilize the affected segments with anterior plating. When resection of one or two vertebral bodies is needed, my first choice is to use mesh and autologous bone to reconstruct the anterior column in conjunction with anterior plating.
Diseases
- Focal facial dermal dysplasia
- Psychosis
- D ercole syndrome
- Deafness enamel hypoplasia nail defects
- Tachycardia
- Convulsions benign familial neonatal
- Oculocerebral hypopigmentation syndrome Cross type
- Hereditary type 1 neuropathy
- Typhoid
Buy cheapest motilium
Reconstruction sagittal computed tomography (A) shows irregularities of L3-4 vertebral end plates and paravertebral extension (B) gastritis enteritis discount motilium 10 mg buy. Sagittal T2-weighted magnetic resonance imaging before (C) and after (D) 4 weeks of therapy with antibiotic, bed rest, and external immobilization shows the lowering L3-4 hyperintensity signal. The diameter of the epidural space is greater at the dorsal portion of the vertebra canal and gradually expands from C7 along the thoracic region, with the greatest depths below L2. The blood value for C-reactive protein was 102, and that for the erythrocyte sedimentation rate was 118. F and G, the infected tissue obtained by fluoroscopy-guided needle biopsy was positive for Staphylococcus capitis. After surgery, the patient had recurrent seroma (I) that was treated by reoperation and multiple sutures of the subcutaneous tissue to the muscle (J) to eliminate the dead space. The abscess suppresses the signal from the cerebrospinal fluid by gadolinium enhancement and can thereby be anatomically localized. Despite clinical improvement, the loss of gadolinium uptake and restoration of bone appear later in the clinical evolution. Despite the improved diagnostic tools and procedures, delay in diagnosis remains an important issue. The goals of treatment are infection eradication, preservation of neurological status, pain relief, prevention of neurological deterioration, and maintenance of vertebral column stability. Many of the cases with an indication for surgery were determined by delay in diagnosis and the subsequent inefficacy of the antibiotic therapy. There is no discussion about the need for surgical treatment in patients with sepsis or burgeoning neurological deficit, but there is some controversy in cases that present with minimal or no neurological findings. Antibiotics are the main therapy for eradication of the underlying infection and should always be prescribed. Antimicrobial therapy can be associated with external immobilization or combined with surgical treatment. When present is small with thick and irregular rim enhancement Rare Usually not observed TuberculousInfection Thoracic and thoracolumbar junction Variable Disk space sparing from severe destruction up to contiguous spread to adjacent vertebral body High bone destruction with multilevel aspects. Late stage with variable intensity in T1 Usually observed in large anterior subligamentous abscesses Frequent. The speed at which antibiotics are initiated following either blood cultures or percutaneous biopsy has dramatically improved the prognosis for recovery and preservation of neurological status such that open surgical decompression should be reserved for patients identified with neurological deficits in the early stages of disease. The presence of neurological deficit plays a predominant role in the treatment algorithm of spinal epidural abscesses, particularly in the early stages of the disease.
10 mg motilium sale
H chronic gastritis forum motilium 10 mg buy, Severe pain, numbness, and weakness caused by progressive thoracic outlet syndrome, manifested as multiple points of sharp distortion of the course of the nerve (arrows) with edema and hyperintensity affecting multiple elements of the brachial plexus. For instance, median nerve entrapment in the distal part of the forearm can lead to failure of treatment if only the flexor retinaculum is addressed. Electrodiagnostic studies can yield misleading results if they are performed under the assumption that abnormalities in certain regions. However, both images are from the same individual and were obtained at the same location in the wrist; they differ only in that one is in a position of flexion and one in extension of the wrist. In a series of patients with clinically and electrodiagnostically confirmed carpal tunnel syndrome, electromyography revealed that although most had compressive lesions, some demonstrated only nerve adhesion with loss of normal mobility of the nerve on flexion and extension of the wrist. From the points of view of electrodiagnosis and surgical treatment, there is little difference between adhesive and compressive carpal tunnel syndrome. Both entities produce similar clinical and diagnostic pictures and respond to the same surgical treatment. However, from the point of view of imaging, it is important to appreciate that patients may have moderate to severe carpal tunnel symptoms with no evidence of nerve compression if adhesion is present. Clinically, this demonstration is of potentially greater importance because in many cases it is possible to demonstrate with imaging that a nerve is not gliding normally across a joint. Restriction of movement of a nerve can cause repeated trauma to the nerve, as well as symptoms of pain exacerbated by extremes of motion or by assuming particular postures or limb positions. The right side (A) demonstrates an S-shaped course passing under the clavicle and over the first rib (arrows), whereas the elements of the brachial plexus on the left side (B) travel along a comparatively straight course (arrow). Lumbar neurography for evaluation of sciatica of nondisk origin caused by entrapment of the lumbar spinal nerve in the distal foramen. A, Normal anatomy of the L3, L4, and proximal L5 nerve roots and lumbar spinal nerves as they exit the spine and travel in essentially linear manner. B, Exiting right L5 nerve root (asterisk) in a 65-year-old woman with persistent right L5 radiculopathy after two spine operations. The course of the exiting root is distorted, and both focal narrowing and a region of L5 spinal nerve hyperintensity (arrow) are apparent. C, Myelogram of the same patient obtained just before magnetic resonance neurography. The L5 root abnormality (asterisk) is too distal to be appreciated on the myelogram, and the study was read as showing a normal L5 root with no impingement. After neurographic diagnosis, the patient underwent distal foraminotomy, which provided excellent lasting relief of the radiculopathy. The nerve is flattened and hyperintense and has expanded to more than twice its normal diameter. This is a postoperative result that occurred when only one of the two bipartite elements of the piriformis muscle was released in a patient with a split nerve and split muscle. Differential retraction of the cut piriformis segment in relation to the intact segment caused a severe mechanical impingement syndrome.

Generic 10 mg motilium with amex
Topiramate in treatment of patients with chronic low back pain: a randomized gastritis diet recipes motilium 10 mg line, doubleblind, placebo-controlled study. Pharmacotherapy of low back pain: targeting nociceptive and neuropathic pain components. Antidepressants in the treatment for chronic low back pain: questioning the validity of meta-analyses. A systematic review on the effectiveness of pharmacological interventions for chronic non-specific low-back pain. Muscle relaxants for nonspecific low back pain: a systematic review within the framework of the Cochrane Collaboration. Comparative efficacy and safety of skeletal muscle relaxants for spasticity and musculoskeletal conditions: a systematic review. A survey of primary care physician practice patterns and adherence to acute low back problem guidelines. Nonpharmacologic therapies for acute and chronic low back pain: a review of the evidence for an American Pain Society/American College of Physicians clinical practice guideline. Massage for low back pain: an updated systematic review within the framework of the Cochrane Back Review Group. Systematic review: strategies for using exercise therapy to improve outcomes in chronic low back pain. Spinal manipulative therapy for chronic low-back pain: an update of a Cochrane review. Effectiveness of acupuncture for nonspecific chronic low back pain: a systematic review and metaanalysis. Growth of spinal interventional pain management techniques: analysis of utilization trends and Medicare expenditures 2000 to 2008. American Society of Anesthesiologists Task Force on Chronic Pain Management, American Society of Regional Anesthesia and Pain Medicine. A critical review of the American Pain Society clinical practice guidelines for interventional techniques: part 2. Outcome of invasive treatment modalities on back pain and sciatica: an evidence-based review. Guideline warfare over interventional therapies for low back pain: can we raise the level of discourse Injection therapy for subacute and chronic low back pain: an updated Cochrane review. Injection therapy and denervation procedures for chronic low-back pain: a systematic review. Response to steroid and duration of radicular pain as predictors of surgical outcome. Transforaminal injection of corticosteroids for lumbar radiculopathy: systematic review and meta-analysis. Epidural corticosteroid injections in the management of sciatica: a systematic review and meta-analysis.
Discount motilium 10 mg mastercard
A bayonet spinal needle is inserted into the disk space and a confirmatory lateral radiograph is performed chronic gastritis with h pylori purchase motilium 10 mg mastercard. The level is then marked with a surgical marker or with electrocautery with attention to the midline. The longus colli is then coagulated at its medial margin with bipolar electrocautery and carefully mobilized with a periosteal elevator in order to avoid Anterior Approach for Cervical Disk Herniation AnesthesiaandPositioning On the day of surgery, the procedure is discussed between the surgeon and the anesthesiologist. It is important to discuss the reason for surgery and the extent of cervical spinal cord compression. When surgery is being performed for radiculopathy in the absence of spinal cord compression, the patient usually will have full range of flexion and extension. In patients who have cervical spondylotic myelopathy, it is useful to ask the patient to flex and extend the neck voluntarily because it helps the anesthesiologist determine a safe zone of extension for intubation. In some circumstances an awake fiberoptic intubation under conscious sedation may be necessary, or the anesthesiologist may chose to utilize a GlideScope (Verathon Inc. The surgeon can make note of patient limitations and limit neck extension during positioning. The expense of routine use of this modality versus the potential mitigation of serious neurological injury must be carefully considered. It is important to pad potential areas of peripheral nerve compression and to make sure intravenous access is not compromised. The lateral aspect of the vertebral body can be palpated and acts as a margin for the extent of lateral dissection. Self-retaining retractors are then placed with either the teeth or the blunt edge beneath the longus colli muscle. An additional rostrocaudal retractor system can be used to improve the exposure and help prevent inadvertent soft tissue injury. Alternatively, Caspar distraction pins can be placed midline at the midpoint of the vertebral body to assist in exposure and help distract the intervertebral disk space. Apfelbaum and associates also recommend deflating the endotracheal tube to "just seal" pressure to help minimize pressure on the anterior soft tissue structures such as the recurrent laryngeal nerve. The drilling trajectory must be kept perpendicular to the vertebral body to avoid skating obliquely and injuring the vertebral artery. The width of the decompression need not extend more than 18 mm, because any radicular symptoms would be addressed at the level of the disk. Although injury to the vertebral artery is uncommon, preoperative imaging should be reviewed to assess for an anomalous course of the artery, especially in patients with other dysmorphic osseous anatomy.
Ashton, 35 years: Therefore, deep-seated tumors are treatable with relative sparing of the superficial tissues. This encouraging result led to the subsequent multicenter phase 2 ProCord trial in Israel and the United States, which included a control group. Lateral and anterior meningiomas, however, may have dural bases that cannot be resected or, if resection is feasible, dural reconstruction is not.
Hassan, 28 years: Long-term results of Gamma Knife surgery for the treatment of craniopharyngioma in 98 consecutive cases. Radiosurgery for spinal metastases: clinical experience in 500 cases from a single institution. There is pain at the time of injection, and there have been reports of a mild flulike syndrome.
Olivier, 65 years: Primary bone tumours of the spine: a 42-year survey from the Leeds Regional Bone Tumour Registry. The design of clinical trials for cell transplantation into the central nervous system. Pulley for strengthening a muscle replacement operation across two joints in brachial plexus lesion: description of the surgical technique.
Vigo, 27 years: In their series, there were no differences in any of the variables studied between the groups treated with antibiotic therapy before or after biopsy. If the difference between arterial pressure measured by cuff and tissue pressure measured by manometer is less than 40 mm Hg, ischemic infarction is likely to occur. On occasion, it has been necessary to make a small laminotomy to visualize the dura directly and confirm puncture.
Volkar, 48 years: Spreading the energy of a treatment out among the beams (current models use either 201 or 192 beams) makes it possible to achieve a high radiation dose within the target volume while largely sparing normal brain, because the dose quickly falls to a low level as the distance from the focus (or isocenter) increases. The needle causes minimal artifact and appears as a black signal void in the image. Evaluation of the spine includes inspection, palpation, and range-of-motion testing.
Riordian, 54 years: International consensus statement on malignant peripheral nerve sheath tumors in neurofibromatosis. Affected bone marrow areas (arrows) are located periarticularly (short tau inversion recovery). Facet cyst in the lumbar spine: radiological and histopathologic findings and possible pathogenesis.
Gunnar, 38 years: The embryologic dysfunction likely involves an idiopathic dilation of the terminal ventricle that disrupts the mesenchymal layer only and then adheres to the overlying skin and prevents spinal cord ascension. It is important to undermine the platysma muscle in order to reduce superficial tension and a restricted surgical field. Single institution experience treating 104 vestibular schwannomas with fractionated stereotactic radiation therapy or stereotactic radiosurgery.
Peer, 39 years: Biomechanical evaluation of destabilization following minimally invasive decompression for lumbar spinal canal stenosis. Without a history of trauma, acute paresis or paralysis of the extremities is most likely related to spinal cord infarction or spinal hemorrhage. Because of advancements in imaging and surgical techniques, the Enneking principles can be safely applied for tumors of the spine.
Runak, 53 years: Obliteration was noted in 5 of 12 patients (42%) having follow-up angiography 3 or more years after radiosurgery. Chapter 330 concludes this block with a discussion of posterior, transforaminal, and anterior lumbar interbody fusion. This treatment was followed by interspinous wiring and cement augmentation to stabilize the involved segment and to arrest the posterior spinal element growth.
Wenzel, 56 years: This capability also provides the opportunity to reduce surrounding tissue toxicity while maintaining a standard therapeutic treatment dose to the target volume. Postoperative imaging invariably shows a small pseudomeningocele that may resolve. In the delayed presentation, rather than attempting primary nerve repair, the surgeon can perform secondary repair with tendon transfers.
Aidan, 58 years: Most importantly, by flattening the entrance to the Alcock canal, the spasmed muscle can cause impingement of the pudendal nerve. A prospective randomized double-blind controlled trial to evaluate the efficacy of an analgesic epidural paste following lumbar decompressive surgery. A comprehensive review of the development of current myoelectric control strategies and future directions.
Innostian, 44 years: Malignant tumors of the axial skeleton are 25 to 40 times more likely to be metastatic than primary. A family history of peripheral nerve problems or any other genetic disorders should be closely questioned, and a history of previous radiation treatments should be discussed. This condition might be caused by the presence of an abnormal fibrous band that originates in an elongated C6 or C7 transverse process and ends at the first rib or the pleural cupola.
Rasul, 36 years: These lesions tend to be less well encapsulated than schwannomas and present as a diffusely expansile lesion of the involved nerve. C, After placement of a series of epineurial sutures on the top side, the lateral sutures are inverted so that the back side of the repair site is exposed and sutured. Impact of dose on local failure rates after image-guided reirradiation of recurrent paraspinal metastases.
Vandorn, 42 years: In 30% of cases, the nerves are sharply transected,4 but in 70% of these injuries, the nerve appears to be in partial continuity (20%) or complete continuity (lesion-in-continuity; 50%). Although radiation is a known cause of meningioma, and there has historically been speculation regarding postirradiation malignant transformation, Strojan and coauthors reviewed the case files of 170,000 meningioma patients treated in Slovenia over a 31-year period and reported the actuarial risk for a secondary meningioma developing after cranial irradiation to be only 0. Moreover, a single tendon, of course, cannot be expected to perform two opposing actions simultaneously.
Knut, 51 years: Seventeen patients had angiographic follow-up at a mean of 21 months after radiosurgery. Pathogenesis of myelopathy in patients with ossification of the posterior longitudinal ligament. Progressive disc herniation: an investigation of the mechanism using radiologic, histochemical, and microscopic dissection techniques on a porcine model.
Ketil, 40 years: Consequently, successful identification of the specific location of the pathology is a critical step to safe, effective surgical management. If properly anticipated, plans can be made to perform the necessary posterior, lateral, or anterior instrumented fusion in the same surgery, which is preferable. Longterm follow-up will determine the efficacy of these stand-alone devices compared to traditional bone-plate constructs.
Iomar, 47 years: For half of these cases, the signs and symptoms are characteristic of rotator cuff injury. Magnetic resonance neurography-surgical correlation of neurologic thoracic outlet syndrome. Magnetic resonance imaging: an accurate method to evaluate arteriovenous malformations after stereotactic radiosurgery.
Cyrus, 59 years: The small size of the spinal cord limits the voxel size and may cause imprecise quantification of metabolite concentrations. The authors of a systematic review concluded that current evidence consistently favors decompressive surgery over conservative treatment for improvements in pain, disability, and quality of life, although not for walking ability. Sprouts from cut corticospinal axons persist in the presence of astrocytic scarring in long-term lesions of the adult rat spinal cord.
Bogir, 25 years: Type I fibers (A) represent the largest caliber axons (13 to 20 �m) with conduction velocities of 80 to 120 m/ sec. They are expansile and, as on imaging, are associated with significant bony destruction with thin layers of reactive cortical bone surrounding them. A retrospective analysis of tumor growth rate, functional hearing preservation, and number s of patients requesting radiosurgery have led to modification of the practice.
8 of 10 - Review by V. Achmed
Votes: 85 votes
Total customer reviews: 85