Sevelamer
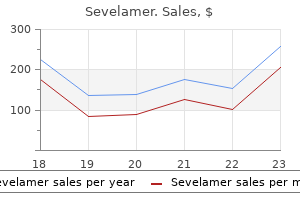
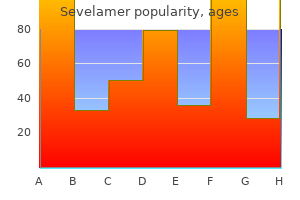
Sevelamer dosages: 800 mg, 400 mg
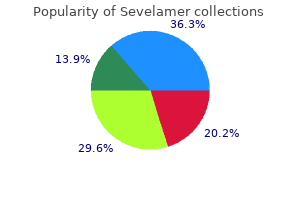
Sevelamer packs: 10 pills, 30 pills, 60 pills, 120 pills, 90 pills

Cheap sevelamer online mastercard
Polyuria may cause bladder distention gastritis vs ulcer symptoms buy sevelamer pills in toronto, hydronephrosis, and permanent renal damage. Although the mortality of patients with hypernatremia is 40% to 55%, it is unclear whether hypernatremia contributes to mortality or is simply a marker of severe associated disease. Surprisingly, if plasma [Na+] is initially normal, moderate acute increases in plasma [Na+] do not appear to precipitate central pontine myelinolysis. However, larger accidental increases in plasma [Na+] have produced severe consequences in children. In experimental animals, acute severe hypernatremia (acute increase from 146 mEq/L to 170 mEq/L) caused neuronal damage at 24 hours, suggestive of early central pontine myelinolysis. Because hypovolemia accompanies most pathologic water loss, signs of hypoperfusion also may be present. In many patients, before the development of hypernatremia, an increased volume of hypotonic urine suggests an abnormality in water balance. Although uncommon as a cause of hypernatremia, isolated sodium gain occasionally occurs in patients who receive large quantities of sodium, such as treatment of metabolic acidosis with 8. Measurement of urinary sodium and osmolality can help to differentiate the various causes. Treatment of hypernatremia produced by water loss requires repletion of water as well of associated deficits in total body sodium and other electrolytes (Table 16-16). Common errors in treating hypernatremia include excessively rapid correction as well as failing to appreciate the magnitude of the water deficit and failing to account for ongoing maintenance requirements 1043 and continued fluid losses in planning therapy. Hypernatremia must be corrected slowly because of the risk of neurologic sequelae such as seizures or cerebral edema. At the cellular level, restoration of cell volume occurs quickly after tonicity is altered; as a consequence, acute treatment of hypertonicity may result in overshooting the original, normotonic cell volume. The water deficit should be replaced over 24 to 48 hours, and the plasma [Na+] should not be reduced by more than 1 to 2 mEq/L/hr for the first few hours and, if the hypernatremia has been present for more than 2 days, no more than 10 mEq/L/day. Once hypovolemia is corrected, water can be replaced orally or with intravenous hypotonic fluids, depending on the ability of the patient to tolerate oral hydration. In the occasional sodium-overloaded patient, sodium excretion can be accelerated using loop diuretics or dialysis. In acute, severe hypernatremia, treatment with venovenous hemofiltration was associated with lower mortality than was calculation of water deficit and infusion of hypotonic fluids. If less filtrate passes through into the collecting ducts, less water will be excreted. Intracellular potassium concentration ([K+]) is normally 150 mEq/L, while the extracellular concentration is only 3.
Cheap sevelamer online amex
The nerves of the plexus converge toward the greater sciatic foramen anterior to the piriformis muscle on the posterior pelvic wall gastritis diet ������� sevelamer 400 mg buy on line. The main terminal nerves are the sciatic nerve (continuation of the plexus) and the pudendal nerves ("terminal branches"). The gluteal vessels (superior and inferior) generally follow the course of the sacral nerves in the anterior plane and can be used to help identify the sciatic nerve at its proximal course. These combined nerves exit through the sciatic notch and pass anteriorly to the piriformis muscle to then lie between the ischial tuberosity and the greater trochanter of the femur. At a variable distance within the posterior thigh (often high in the popliteal fossa), the sciatic nerve bifurcates into the tibial and common peroneal nerves. The common peroneal nerve descends along the medial border of the biceps femoris muscle and then on the lateral border of the gastrocnemius muscle. At the fossa, it gives off the lateral sural nerve, which forms the lateral sural cutaneous nerve by joining the medial sural nerve supplied by the tibial nerve. It winds around neck of the fibula and terminates as the deep and superficial peroneal nerves. In the posterior thigh, the tibial nerve is covered medially by the semitendinosus and semimembranosus muscles and 2381 laterally by the biceps femoris muscle. Beyond the knee joint, it is covered by both heads of the gastrocnemius muscle and then deep to the soleus muscle, before coming to an end on the tibialis posterior muscle and finally on the posterior surface of the tibial shaft medial to the medial malleolus. Within the fossa, it gives off muscular branches (gastrocnemius, soleus, popliteus, and plantaris muscles) as well as the medial sural nerve (to join its lateral counterpart from the common peroneal nerve). In the lower leg and foot, it gives off muscular, articular (ankle), and cutaneous branches and terminates as the medial and lateral plantar nerves. Terminal Nerves of the Lumbar Plexus Genitofemoral Nerve (L1, L2) this nerve leaves the lumbar plexus at the lower border of the L3 vertebra. It pierces and then lies anterior to the psoas major muscle before descending subperitoneally and behind the ureter, where it divides into two branches (genital and femoral) at a variable distance above the inguinal ligament. The genital branch crosses the external iliac artery and traverses the inguinal canal. It supplies the cremaster muscle and skin over the scrotum and adjacent thigh (males) or the skin over anterior part of labium majus and mons pubis (females). The femoral branch descends lateral to the external iliac artery, passes under the inguinal ligament, enters the femoral sheath lateral to the femoral artery, and pierces the anterior layer of the femoral sheath and fascia lata. It innervates the skin immediately below the crease of the groin anterior to the upper part of the femoral triangle.
800 mg sevelamer buy mastercard
Modern pulse oximeters are noninvasive gastritis vinegar buy sevelamer 400 mg without a prescription, continuous, autocalibrating, have quick response times, and are suitable for use during transport. However, pulse oximetry is a poor indicator of adequate ventilation; desaturation is a late sign of apnea or respiratory insufficiency. Monitoring of expired carbon dioxide is now recommended for procedures involving moderate to deep sedation in addition to procedures performed under general anesthesia. Advances in infrared absorption spectroscopy have led to the production of conveniently portable devices for expired gas analysis. During direct invasive arterial pressure monitoring, the fidelity of the system is optimized when the catheter and tubing are stiff, the mass of the fluid is small, and the length of the connecting tubing is not excessive. Automated noninvasive blood pressure monitors use the oscillometric method to estimate arterial blood pressure. Pulsatile flow generates oscillations in the internal pressure of an inflated blood pressure cuff; these oscillations are greatest when the cuff is inflated to mean arterial pressure. During prolonged surgical cases, it may be prudent to relocate the blood pressure cuff every few hours to reduce the risk of neurapraxia or cutaneous injury. Clinical studies have demonstrated that patients in whom intraoperative hypothermia develops are at a higher risk for development of 1760 postoperative myocardial ischemia and wound infection compared with patients who are normothermic in the perioperative period. Although liquid crystal skin temperature strips are convenient to apply, they do not correlate well with core temperature measurements. On the contrary, it requires anesthesiologists to understand the operation of these devices intimately so that they can be used safely, accurately, and appropriately. Introduction Historically, the foundation of anesthesia practice has been vigilance and ongoing clinical examination of the patient. The development of modern monitoring equipment does not replace these responsibilities. Automated monitoring equipment provides the anesthesiologist with the ability to acquire clinical information either more rapidly or more frequently than can be achieved through manual techniques or in a more quantitatively precise manner than can be achieved by physical examination alone. The purpose of monitoring equipment, then, is to augment the situational awareness of the anesthesiologist so that clinical problems can be recognized and addressed in a timely manner and to guide treatment. The term itself is derived from monere, which in Latin means to warn, remind, or admonish. This chapter discusses the methods and biomedical devices through which anesthesiologists monitor the physiologic state of the patient during anesthesia care. These explanations are, by necessity, simplified, as the actual design of a biomedical device involves significant engineering complexity. However, the explanations are intended to be sufficient to allow the anesthesiologist to understand how the device acquires its clinical data and how that process might be compromised and the data made erroneous as well as to understand how the device works and how it may fail. There is little high-grade evidence that electronic monitors, by themselves, reduce 1761 morbidity and mortality.
800 mg sevelamer purchase mastercard
Pain from a symptomatic protrusion of a cervical disk can be intensified unless the head is carefully positioned so that lateral or ventral flexion gastritis symptoms diarrhoea purchase sevelamer with amex, extension, or rotation is avoided. Suprascapular Nerve Ventral circumduction of the dependent shoulder can rotate the suprascapular notch away from the root of the neck. Because the suprascapular nerve is fixed both paravertebrally and at the notch, circumduction can stretch the nerve and produce troublesome, diffuse, dull shoulder pain. The diagnosis is established by blocking the nerve at the notch and producing pain relief. Treatment may require resecting the ligament over the notch to decompress the nerve. A supporting pad placed under the thorax caudad of the axilla and thick enough to raise the chest off the shoulder may prevent a circumduction stretch injury to the nerve. Wrapping the legs in compressive bandages, or the use of fulllength elastic hosiery, minimizes pooling of blood in distensible vessels and supports venous return. Parallel chest rolls extended from just caudad of the clavicle to just beyond the inguinal area, with a pillow over the pelvic end. The head is turned onto a C-shaped pad, gel, or foam sponge that frees the downside eye and ear from compression. C: Table flexed to reduce lumbar lordosis; subgluteal area straps placed after the legs are lowered to 2028 provide cephalad thrust and prevent caudad slippage. When this position results in the head being lower than the heart, the pressure gradient can result in venous and lymphatic stasis in the head. This position may result in facial and airway edema, making extubation of intubated patients challenging, especially after prolonged procedures such as spine fusions. In addition, over the past decade or two, long spine surgical procedures have resulted in a surprising number of patients who experience severe vision loss. Although the etiology of the ischemic optic neuropathy is not entirely clear, Lee et al. This congestion, added to the effect of gravity on the suspended globe of the eye, can result in optic nerve stretch and possibly the development of ischemic neuropathy (see later). Of these, the Wilson frame is particularly concerning in that its use results in the head being lower than the heart, potentially contributing to optic nerve congestion. The choice of equipment is based on the physique of the patient, the requirements of the surgical procedure, and availability. Pronated patients with limited mobility of the neck, a history of postural neck pain, or a history suggesting a symptomatic cervical disk should have their heads retained in the sagittal plane, either with a skull-pin head clamp or with a face rest.
Sevelamer 800 mg order line
Increased awareness of fire hazards in the operating room environment further reinforces the need for careful monitoring of FiO2 in pediatric anesthesia gastritis definition symptoms order 400 mg sevelamer with mastercard. Tonsillectomy and adenoidectomy, among the most common of surgical procedures in the pediatric anesthesia population, carry an increased risk of airway fire. In addition to using of cuffed endotracheal tubes, careful monitoring and maintenance of a decreased inspired oxygen concentration whenever electrosurgical equipment is in use may decrease airway fire risk in these patients. On the steep part of the curve, a predictable correlation exists between SaO2 and partial pressure of oxygen (PaO2). In this range, the SaO2 is a good reflection of the extent of hypoxemia and the changing status of arterial oxygenation. For PaO2 greater than 75 mmHg, the SaO2 reaches a plateau and no longer reflects changes in PaO2. Coexisting medical conditions, such as hypercapnia, acidosis, and hyperthermia, cause the oxyhemoglobin dissociation curve to shift to the right and decrease the affinity of hemoglobin for oxygen. The change in color results from the optical properties of hemoglobin and its interaction with oxygen. The ratio of oxyhemoglobin (HbO2) and hemoglobin (Hb) can be determined by absorption spectrophotometry. At a constant light intensity and hemoglobin concentration, the intensity of light transmitted through a tissue is a logarithmic function of the oxygen saturation of Hb. Light-emitting diodes in the pulse sensor emit red (660 nm) and near infrared (940 nm) light. The percentage of HbO2 is determined by measuring the ratio of infrared and red light sensed by a photodetector. Pulse oximeters perform a plethysmographic analysis to differentiate the pulsatile "arterial" signal from the nonpulsatile signal resulting from "venous" absorption and other tissues, such as skin, muscle, and bone. The relationship between arterial saturation of hemoglobin and oxygen tension is represented by the sigmoid-shaped oxyhemoglobin dissociation curve. When the curve is left-shifted, the hemoglobin molecule binds oxygen more tightly. The appropriate use of pulse oximetry necessitates an appreciation of both physiologic and technical limitations. Despite the numerous clinical benefits of pulse oximetry, other factors affect its accuracy and reliability. Factors that may be present during anesthesia care and that affect the accuracy and reliability of pulse oximetry include dyshemoglobins, dyes (methylene blue, indocyanine green, and indigo carmine), nail polish, ambient light, lightemitting diode variability, motion artifact, and background noise.
Buy sevelamer on line amex
The reason for this discrepancy is that although the overhead costs in a small office are usually quite reasonable and managed gastritis symptoms lap band cheap 800 mg sevelamer otc, the comparable costs in a large tertiary care hospital can be both enormous and unforseen. When the same procedure was performed in an office, the price was decreased to $1,534. Similarly, the average cost of an inhospital open inguinal 2142 hernia repair that same year was found to be $2,237, whereas only $894. It is understandable that insurance companies now offer incentives to surgeons who utilize an office location as their preferred surgical venue. These usually relate to patient safety, reporting, quality improvement, and peer review. However, the number of such states without regulation and oversight is rapidly decreasing (Table 32-1). In fact, the remote location of an office may specifically confer an increased risk of injury during an office-based anesthetic. Reasons include toxicity of local anesthetics; prolonged surgery with occult blood loss; pulmonary embolism; and accumulation of multiple anesthetics resulting in oversedation, hypovolemia, hypoxemia, and the use of reversal drugs with short half-lives. Since the majority of office-based patients are young and healthy, one would expect that anesthetics performed in offices would be at least equally as safe as those performed in hospitals, if not safer. They had a 57% response rate and found that over a 5-year period, 400,675 office procedures were performed; of these, 63. Several outcomes were reviewed including hemorrhage, hypertension, hypotension, wound infection, and need for hospital admission and reoperation. A close look at the more recent data again supports the supposition that an office-based procedure is as safe as a procedure done in a more traditional setting. They concluded that there is no increase in mortality for an ambulatory setting when compared to a freestanding hospital. One important caveat when looking at safety records for office-based surgery is that there are no prospective randomized studies. When examining the literature, it becomes clear that there have been several studies that report a poor outcome for patients undergoing office-based procedures. Some more recent data have shown that office-based morbidity and mortality are usually the result of inadequate perioperative patient monitoring, oversedation, and thromboembolic events. In addition, although an anesthesiologist may not even be administering the anesthetic in an office, many complications may still be reported as anesthetic-related. For example, traditional credentialing procedures, such as board certification and the granting or renewing of hospital privileges based on competency and proof of continuing medical education, may not be required or enforced in an office. Within and among offices, providers of anesthesia may also have varying degrees of both education and expertise. The provider may be an anesthesiologist, a nurse anesthetist, a dental anesthetist, or a surgeon with little or no training in anesthesia. Furthermore, safety within an anesthetizing location also depends on the perioperative patient monitoring capabilities.
Buy sevelamer 400 mg amex
This is a high-efficiency intrinsic-pathway "tenase gastritis symptoms vs gallbladder buy generic sevelamer canada," which provides many times more Xa for more prothrombinase complex. Ultimately, thrombin cleaves fibrinogen to fibrin monomers, which then polymerize extensively. Inhibition of Clotting Factors 1092 the clotting pathways have three main regulatory inhibitors. Serpins disrupt the active sites and increase the clearance of their target proteases. Protein C-ase is an enzymatic complex with the same four-part structure as the coagulation complexes above: an enzyme, thrombin, its cofactor thrombomodulin, phospholipid, and Ca2+. Urokinase is secreted from the endothelium, monocytes, macrophages, and urinary epithelium. These cells also bind plasminogen with two receptors, the annexin A2 complex and the urokinase receptor, which facilitate its conversion to plasmin. Clear chevron: antifibrinolytic medications blocking the lysine-binding sites on plasminogen. These drugs are lysine analogues that block the lysine-binding sites of plasminogen, preventing it from acting on fibrin. The family history is helpful in diagnosing a congenital problem and the possible pattern of inheritance. Anticoagulants and antiplatelet medications, including over-the-counter drugs, should always be reviewed before ordering laboratory analysis. Laboratory Evaluation of Primary Hemostasis the normal automated platelet count in adults is approximately 150,000 to 400,000/L. The peripheral blood smear should be examined in specimens with abnormal platelet counts. Microscopic review may reveal clotted specimens, artifactual platelet clumping in vitro, or abnormal platelet morphology. However, this test is invasive, labor-intensive, impractical to repeat frequently, poorly reproducible, and only modestly predictive for bleeding problems. In contrast, when both pairs are abnormal, other congenital or acquired platelet dysfunctions may be present. False negatives are common and abnormal results can also be caused by thrombocytopenia, uremia, or anemia. Several other devices test for specific antiplatelet medication effects from aspirin or P2Y12 inhibitors. Some uncommon congenital disorders lack responses to specific agonists in a characteristic fashion. More detailed testing may be needed for a specific diagnosis, such as electron microscopy for granule defects, flow cytometry for surface receptors and granule markers, or genetic testing.
Buy discount sevelamer line
Perioperative plasma volume expansion reduces the incidence of gut mucosal hypoperfusion during cardiac surgery gastritis symptoms fever order sevelamer 800 mg with amex. Intraoperative intravascular volume optimisation and length of hospital stay after repair of proximal femoral fracture: randomised controlled trial. Esophageal Doppler ultrasound monitor versus pulmonary artery catheter in the hemodynamic management of critically ill surgical patients. Esophageal Doppler monitor determinations of cardiac output and preload during cardiac operations. Randomized controlled trial to investigate influence of the fluid challenge on duration of hospital stay and perioperative morbidity in patients with hip fractures. Early goal-directed therapy in severe sepsis and septic shock revisited: concepts, controversies, and contemporary findings. Prospective, randomized trial comparing fluids and dobutamine optimization of oxygen delivery in high-risk surgical patients. Supranormal trauma resuscitation causes more cases of abdominal compartment syndrome. Spironolactone versus eplerenone for the treatment of idiopathic hyperaldosteronism. Risk of hyponatraemia in cancer patients treated with targeted therapies: a systematic review and meta-analysis of clinical trials. Correction of hyponatremia and osmotic demyelinating syndrome: have we neglected to think intracellularly Upregulation of aquaporin-2 water channel expression in chronic heart failure rat. Copeptin in the diagnosis of vasopressin-dependent disorders of fluid homeostasis. Copeptin as a biomarker and a diagnostic tool in the evaluation of patients with polyuria-polydipsia and hyponatremia. A randomized controlled trial of hydrocortisone against hyponatremia in patients with aneurysmal subarachnoid hemorrhage. Fatal central diabetes mellitus and insipidus resulting from untreated hyponatremia: a new syndrome. Postoperative hyponatraemic encephalopathy following elective surgery in children. A copeptin-based classification of the osmoregulatory defects in the syndrome of inappropriate antidiuresis. Hyponatremia: current treatment strategies and the role of vasopressin antagonists.
Khabir, 64 years: Muscular dystrophy patients with preoperative muscle weakness may require postoperative mechanical ventilation.
Sulfock, 56 years: Early cadaveric studies showed that correctly applied cricoid pressure was effective in preventing gastric fluids from leaking into the pharynx.
Curtis, 27 years: Color Doppler may be used to identify and avoid the inferior epigastric vessels that run through the rectus muscle.
Armon, 49 years: It is usually transient, inconsequential, and requires only reestablishment of the normal tissue perfusion gradients of the supine position, or of a slight amount of head-up tilt, to be redistributed.
Ernesto, 54 years: Manipulation of the Glidescope to the position needed for adequate image can cause cervical segment extension, though.
Rendell, 34 years: This causes a decrease in pressure 1693 within the circuit, and as a result, the reservoir bag deflates.
Flint, 61 years: Other risk factors for the development of osmotic demyelination syndrome include alcoholism, poor nutritional status, liver disease, burns, and hypokalemia.
Zuben, 36 years: The tip of the Tuohy needle (90 mm, 17 to 20 gauge) should be directed laterally to allow the catheter to run in the direction of the nerves.
Sanford, 62 years: In 1993, with the introduction into clinical use of desflurane, an even more sophisticated vaporizer was introduced to handle the unique physical properties of this agent.
Wenzel, 42 years: Perioperative use of transesophageal echocardiography by anesthesiologists: impact in noncardiac surgery and in the intensive care unit.
Barrack, 23 years: Cerebral blood flow remains constant above an arterial oxygen partial pressure (PaO2) of 50 mmHg (red).
Arokkh, 30 years: Risk factors associated with fast-track ineligibility after monitored anesthesia care in ambulatory surgery patients.
Peratur, 53 years: Unfortunately, sector depth must be reduced because pulse repetition frequency is inversely related to the sector depth, as a longer period of time is required for the ultrasound to travel the increased distances.
Shakyor, 50 years: Relative effects of intrathecal administration of fentanyl and midazolam on A delta and C fibre reflexes.
Narkam, 55 years: As such, neuroanesthesia is the provision of anesthesia and analgesia for a multitude of procedures, including invasive, minimally invasive, neurodiagnostic, and neurointerventional procedures, and involving the brain, spinal cord, and peripheral nerves.
Jaffar, 29 years: A small incision is made in the lateral chest wall, and with the insertion of the instrument, fluid and biopsy specimens are easily obtained.
Vibald, 65 years: Early signs of unintended intrathecal local anesthetic injection can be subtle and easily missed.
9 of 10 - Review by V. Sancho
Votes: 40 votes
Total customer reviews: 40