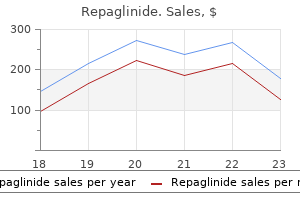
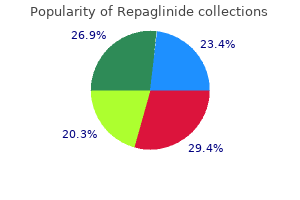
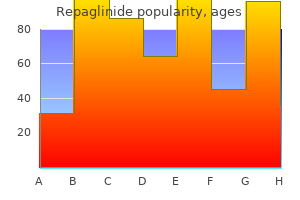
Repaglinide
Repaglinide dosages: 2 mg, 1 mg, 0.5 mg
Repaglinide packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Discount 0.5 mg repaglinide fast delivery
Recent literature suggests that a comprehensive evaluation to assess for the presence of a splenic injury requires both arterial and portal venous phases diabetes in toddlers buy repaglinide master card. The arterial phase performs better for the detection of splenic pseudoaneurysms, and portal venous phase has improved detection for parenchymal lacerations and active bleeding over arterial phase alone. The spleen is the most common region of isolated active extravasation of contrast; however, fractures of the pelvic ring are most commonly associated with multiple sites of extravasation. There is active contrast extravasation seen on arterial phase (A, arrow), which enlarges on 5 minute delayed phase (B, arrows) compatible with active bleeding. There is retroperitoneal gas due to a full thickness duodenal injury (A, arrow head). Active bleeding from the mesentery and an associated small bowel perforation was identified at surgery. The detection of lacerations that extend to the hepatic veins is of particular importance in the liver, as these have a strong predictive value for failure of nonoperative management when associated with large (>10 cm) hypoperfused regions. White arrow shows median fracture of horseshoe kidney with posterior perinephric hematoma (asterisks). This is arterial phase image because there is dense opacification of aorta directly posterior to neck of horseshoe kidney without opacification of the inferior vena cava immediately to its right. Posterior wall of bladder is irregular with double densities within urine contrast compatible with hematoma (arrowheads). Thus, open communication with the interpreting radiologist is recommended to avoid any miscommunication. Although rib fractures are not shown on current image, subcutaneous emphysema in left chest wall and distal extent of small pneumothorax are shown. Administration of dilute water soluble contrast via low gravity drip can proceed only after the positioning of the Foley catheter within the bladder is confirmed. It is not uncommon for a Foley catheter to be inserted through a laceration of the bladder dome in a patient with an intraperitoneal bladder rupture. The relatively uniform enhancement of hepatic parenchyma suggests that the hepatic veins are not occluded. Such through-and-through fractures are typically associated with biomechanical instability. Review of the images using "bone" windows may make the identification of the source of urinary leak more apparent, depending on the density of the contrast material in the bladder. Striated nephrogram is present posteriorly (white arrow), compatible with contusion adjacent to laceration. Unfortunately, the specific signs of a bowel perforation are relatively uncommon and are not sensitive.
1 mg repaglinide purchase visa
Therefore blood glucose safe zone generic repaglinide 1 mg amex, one sees a patient with a drastically rising bilirubin with relatively normal liver function tests. Another method of control included placement of a constant suction T tube with subsequent resolution. Many persistent fistulae may, however, manifest from smaller radicals, which retract into the liver parenchyma and are not visualized. Drain placement at the time of laparotomy is usually indicated with obvious bile staining. It is common for liver injuries to have transient early postoperative serosanguinous and bilious drainage. Bilious drainage of at least 50 mL/d that continues after 2 weeks is considered a biliary fistula. Major left or right bile duct injury often requires further intervention for closure. In the past the surgical approach was recommended with resection or Roux-en-Y procedures predominating. Percutaneous stenting of injuries and drainage of biloma collections has been utilized. At the Shock Trauma Center, Dabbs et al found that 29 of 30 patients encountered with major hepatic necrosis underwent initial operative intervention and 87% underwent damage control laparotomy. A large number of these patients then required resection of their necrotic hepatic parenchyma. Both serial debridements and formal lobectomy were performed, but lobectomy was associated with fewer procedures overall and a lower complication rate. Though it is a rare complication, identification and management can prevent the morbidity of progression to bronchobiliary fistula, which leads to a protracted and complicated clinical course. Often the patient does well initially with resolution of hemothorax, no evidence of jaundice, and stabilization of liver injury only to become significantly tachypneic a week or more later. Rothberg et al promote operative intervention in order to evaluate for significant diaphragmatic injury, liver necrosis, or lung necrosis with possible bronchial involvement. Technical problems including continued hemorrhage, adjacent organ injury, and small duct size can prove difficult. A timely diagnosis and treatment method may prove to be the survival difference in patients with these severe injuries. In a Seattle paper, 38% were a result of blunt mechanisms, similar to the 31% with blunt mechanism quoted in a 1995 multi-institutional trial. When examining those with both portal vein and hepatic artery injury, the mortality is 99%. Instead, multiple injuries to the liver, porta, vena cava, and surrounding viscera most often occur. Not only are these portal triad injuries difficult to manage, but also the specific injury cannot be identified preoperatively, therefore, intraoperative decision making is crucial.
Generic 1 mg repaglinide overnight delivery
Vitreous hemorrhage is invariably present in eyes with scleral rupture and may be present in penetrating injuries diabetes mellitus in pregnancy best buy repaglinide. In closed globe injury, it may be associated with iris sphincter tears, hyphema, and lens dislocation, while in the posterior segment associated findings include retina tear/ detachment, traumatic macular hole, choroidal rupture, and traumatic optic neuropathy. If the severity of the vitreous hemorrhage does not allow sufficient visualization of the retina, B-mode ocular echography to detect retinal tears or detachment can be utilized as an acceptable alternative to direct visualization. It should be noted that when the vitreous hemorrhage is very severe, it is impossible to reliably detect a retinal detachment. Spontaneous resolution is the rule with the long-term prognosis determined by concomitant retinal pigment epithelium injury. Contusion of the retinal pigment epithelium is infrequently described, yet it is a common sequela of closed globe injury characterized by atrophic changes and mottling of the retinal pigment epithelium in the long term. The difference between retinal tears and dialyses is beyond the scope of this text but is significant when considering surgical repair of a detachment. Following closed globe injury, the sudden expansion of the equatorial region of the eye results in the forced separation of the vitreous from the retina; in young individuals the vitreous may adhere strongly to the retina and its forced separation may result in tears in the retina or retinal dialysis. Usually vitreous hemorrhage (which can be very minor) occurs concomitantly due to bleeding from the vascular retina. In about 85% of patients with retinal tears or dialyses fluid passes under the tear/dialysis causing the retina to float away from the choroid, which is a retinal detachment. If the retinal detachment advances to include the fovea, patients will also report blurred vision. Timely treatment of retinal tears with laser retinopexy (or cryopexy) to reinforce the adhesion between retina and retinal pigment epithelium will prevent retinal detachment. If a retinal detachment occurs, timely treatment (before the fovea is involved) can lead to preservation of excellent vision-therefore, a retinal detachment not involving the fovea needs to be repaired within 24 hours. Once the fovea is involved, the vision will never be normal; patients presenting with fovea-involving retinal detachments need to undergo repair within 1 week of presentation. When retinal detachments are not treated promptly, proliferative vitreoretinopathy (a process of scar formation in the vitreous cavity) supervenes and surgical outcomes are poorer (both anatomic and visual outcomes) and there is a greater risk of phthisis bulbi (globe becoming shrunk with opacification of the cornea). Treatment of retinal detachments is by scleral buckling if the cause is a dialysis, pars plana vitrectomy if there is a giant retinal tear, and pars plana vitrectomy or scleral buckling if the cause is a retinal tear. Moreover, a hemorrhagic retinal detachment may arise from bleeding Chapter 20 Eye 413 under the retina. It should be noted that development of a traumatic macular hole may be delayed by a few days or weeks following trauma. Sadly, we have seen several patients over the years misdiagnosed as having only traumatic iritis, which rarely would present with hypopyon or severe tenderness. Endophthalmitis is a true ophthalmic emergency and in the case of virulent microorganisms such as Bacillus a few hours can make the difference between retaining the globe and losing it to phthisis.
Discount repaglinide express
Performing esophagography on intubated and/or sedated patients is technically challenging diabetes insipidus low specific gravity purchase repaglinide 1 mg without a prescription. A nasogastric tube is necessary to perform this examination on Chapter 15 Diagnostic and Interventional Radiology 267 uncooperative patients. The radiologist manipulates the nasogastric tube to the distal esophagus, and, under real time fluoroscopic surveillance, injects the contrast agent in an attempt to achieve full distention of the esophagus. Care should be taken to avoid over distention of the proximal esophagus, which can result in reflux and aspiration, even in intubated patients. Liberal use of a dedicated 3D volume viewing station for manipulation of the data set is strongly encouraged, as it is often the case that a cervical vascular injury may be best visualized and displayed using nontraditional planes. Catheter angiography is indicated emergently in patients with an expanding cervical hematoma, active extravasation from the nose, mouth, or ears, or a cervical bruit in individuals younger than 50 years old. As such, any patient with "hard" signs of a cervical vascular injury (such as expanding pulsatile hematoma, active bleeding from the wound, hemorrhagic shock, etc. Gunshot wounds can result in significant soft tissue cavitation that may result indirect or indirect vascular injuries. The right common carotid artery is not opacified (arrow) due to injury and subsequent thrombosis. A tracheal defect (arrow head) is present, along with extensive cervical emphysema. Neck zonal anatomy is an important consideration for patients with "hard" clinical signs of significant internal injury (see Chapter 41); however, it should be noted that clinically significant internal injuries may be present in a zone differing than that of the physical examination, and that penetrating wound tracts may extend beyond the neck into the skull base, cranial vault, mediastinum or upper thorax. There are numerous vessels at risk, including the internal carotid artery, the external carotid artery and branches, the vertebral artery, and the accompanying veins. Indeed, arteriography is so valuable for the evaluation and treatment of bleeding in this zone that aggressive steps to resuscitate the unstable patient and control bleeding by packing are warranted to allow angiography to proceed. If the common carotid artery or the internal jugular vein require repair, operative exposure is relatively simple and unobstructed. Thus, little imaging is necessary after penetration when "hard" signs of a vascular injury (see Chapter 41) are present. The detection and treatment of vascular injuries in asymptomatic patients is more controversial. In Zone I, the area inferior to the manubrium of the sternum, the brachiocephalic vessels, trachea, or esophagus may be injured, and rapid exsanguination may occur.
Generic repaglinide 2 mg without a prescription
For example diabetes insipidus for nurses 1 mg repaglinide buy fast delivery, the distribution of injuries related to road traffic has been shown to vary by country, with pedestrians and drivers of two-wheel vehicles found to be particularly vulnerable in certain low and middle income countries. In high income countries, a cornerstone of these systems has been hospital-based trauma registries, a surveillance tool which is increasingly used in low and middle income countries. In Thailand, enactment of a helmet law was associated with a fivefold increase in helmet use among motorcyclists and a concomitant reduction in head injuries by 41% and deaths by 21%. This public health problem was addressed through a combination of legislation, social marketing, and enforcement, and was ultimately associated with significant decreases in injury events, serious injuries, and deaths captured through hospital and police data sources. The Lancet Journal created a Commission on Global Surgery, representing contributions from 110 countries. This resulted in a series of reports, publications and recommendations to guide improvements toward equitable access to affordable surgical care globally. As part of the Road Safety in 10 Years project, enforcement campaigns advocating for seat belt use and speed control in several low and middle income countries have shown promise both in increased utilization and decreased injuries. For example, implementing a helmet law in combination with a seatbelt law in the same region would not only result in a greater reduction in injuries and deaths, but be more cost-effective than only one of these interventions. This is because the infrastructure for enforcing one intervention is shared by the other, mitigating the cost. A community-based intervention in Bangladesh that involved both education and integration of playpens and door barriers for infants found that families who were provided the intervention improved their child supervision practices. Not only were both programs associated with a decreased risk of drowning among enrolled children, but the programs were found to be cost-effective both individually and as a combined intervention. This intervention was associated with significantly decreased odds of both death and complications after implementation. Particularly in high income countries, prevention measures against active and passive injury have been successful in increasing the safety of road users, populations at risk for falls or burns, and potential victims of violent injury. Through comprehensive evaluations and the right mix of fidelity and adaptability, efforts in decreasing both intentional and unintentional injury are demonstrating intermediate and long-term successes. With over 90% of injury deaths occurring in low and middle income countries, appropriate attention is now shifting to worldwide surveillance and strategic planning for injury prevention. Surgeons have a unique opportunity to participate in all components of prevention from surveillance to programming to evaluation and advocacy. Surgeons see patients during that unique "window of opportunity" after injury, making them powerful advocates not only to individuals and community organizations, but to legislators, as well. The injury event, and similarly the hospital itself, is a promising portal of entry into prevention programs. Surgeons have spearheaded projects that have clarified the mechanisms of particular injuries and have implemented and studied programs that can have impact. Surgeons are a vital partner in the multidisciplinary approach necessary to make an appreciable difference in injury-related death and disability globally.
Syndromes
- Weakness
- Choose lean proteins, such as chicken, fish, beans, and legumes.
- Drinking too much fluid
- Burns
- Throat pain
- Where to buy diabetes supplies and how to store them
- Radiation injury to the bowel
- Convulsions
- The part of the device places in the brain may break off or move to a different place in the brain (this is rare)
- Tonsillitis
Cheap repaglinide 1 mg without prescription
The most suitable veins are at the wrist diabetic diet bread 1 mg repaglinide for sale, the dorsum of the hand, the antecubital fossa in the arm, and the saphenous in the leg. For this reason, the incidence of complications is higher and the rate of success is lower in these situations. Subclavian or femoral vein catheterization usually provides rapid and safe venous access in experienced hands. Pneumothorax is more likely to occur on the left side because the left pleural dome is anatomically higher. Trauma patients can be categorized into three general groups with respect to their response to resuscitative maneuvers. Thrombophlebitis or line infection is more common with femoral catheters; however, this is most common with prolonged use. A simple pneumothorax may result in respiratory compromise in individuals with pulmonary contusions or a pneumothorax in the contralateral hemithorax. Regardless of the site of insertion, it is extremely important not to force the wire or the introducer if resistance is encountered. Forcing the introducer could result in perforation of large central veins or arteries and bleeding. Large volume resuscitation with normal saline produces or enhances the frequently present detrimental hyperchloremic metabolic acidosis. Similarly, the use of hypertonic saline as a first-line resuscitative fluid is not recommended. At this time, there is no evidence to endorse use of this fluid for resuscitation. Damage Control Resuscitation There is significant evidence that the best resuscitative fluid for a person in persistent or severe hemorrhagic shock is not crystalloid nor colloid but in fact, a balanced infusion of blood components to mimic, as possible, replacement of fluid lost, that is, whole blood (see Chapter 13). This approach can potentially increase bleeding by elevating the blood pressure and dislodging established blood clots. Hypotensive resuscitation is not a new concept; in 1918, Cannon et al described the deleterious effects of injecting fluids before the surgeon could achieve vascular control of the injury. This approach was primarily an attempt to minimize transfusion volume and blood loss in the operating room. Bickell et al in 1994 published a prospective analysis comparing immediate and delayed fluid resuscitation in hypotensive adult trauma patients with penetrating torso injuries in the city of Houston. Improved survival was seen in this study population, with a trend toward fewer complications. These data corroborated the concept that delaying fluid resuscitation until hemorrhage is controlled improves outcome in this select group of penetrating trauma patients.
Discount 0.5 mg repaglinide free shipping
This involves the administration of both a sedating agent and a neuromuscular blocking agent prior to endotracheal intubation signs diabetes rabbits discount repaglinide 0.5 mg buy on-line. In skilled hands, this technique can facilitate effective airway control in patients when other methods fail or are otherwise unacceptable (eg, the patient with trismus). Wang and Yealy72 reviewed the data on prehospital intubation and concluded that there is little literature to support maintaining endotracheal intubation as the standard airway of choice. Most children can maintain adequate oxygenation/ventilation with bag valve mask assistance and do not necessarily require endotracheal intubation. Although various models differ in design, properly positioned devices have openings that allow for passage of air from the device into the adjacent glottic opening to ventilate the lungs. This device is blindly inserted into the hypopharynx so that the ring seals around the glottic opening. This device has replaced endotracheal intubation for general anesthesia in a significant percentage of shorter operations, especially in Great Britain. A potential disadvantage of these devices is that the risk of aspiration is believed to be greater than with endotracheal intubation. Supraglottic devices are valuable backup ("rescue") airways when endotracheal intubation cannot be accomplished. Because of the controversies with endotracheal intubation, these airways are increasingly utilized as the initial airway of choice, although these airways can be problematic because of potential risks. Use of either endotracheal intubation or a supraglottic airway is a low-volume, high-risk procedure and requires rigorous medical oversight. Needle Jet Insufflation this involves the insertion of a large-bore needle through the cricothyroid membrane and connecting it to high-pressure oxygen. This technique possesses the following advantages: it does not require paralysis, is less invasive than surgical cricothyroidotomy, affords easy access and insertion, and requires minimal education and very basic equipment. The technique has been demonstrated experimentally to be safe and effective even in the presence of complete obstruction of the airway. While oxygenation is adequate, studies have shown that the patient may become hypercarbic. Surgical Cricothyroidotomy this involves incising the skin and the cricothyroid membrane, followed by the insertion of a small endotracheal or tracheostomy tube. Because it is highly invasive, complications have included significant hemorrhage and injury to adjacent nerves, blood vessels, and the larynx. Air medical crews have utilized surgical cricothyroidotomy in the prehospital setting for several decades with good success. Use of this procedure by out-of-hospital personnel requires strong medical oversight and intense training. Auscultation of breath sounds should be performed during the primary survey if the patient has an abnormal ventilatory rate or evidence of respiratory distress. Pulse oximetry should be monitored, and oxygen administered to maintain an Spo2 of at least 90% if not more. Prehospital care providers must exercise caution while providing ventilatory support, as deleterious effects may ensue.
Buy repaglinide 0.5 mg with visa
When all attempts to close the fascia have failed diabetes definition dictionary.com generic 2 mg repaglinide visa, complex closure methods with mesh may be utilized. The temporary abdominal closure ideally will contain the viscera, protect the bowel, provide early identification of intra-abdominal complications, and preserve healthy fascia for subsequent closure. There are a variety of techniques utilized to perform temporary abdominal closure. Utilization of towel clips to being the skin together is the simplest and fastest method. A running suture in the skin is another easy method to bring the skin together, but takes longer to apply. Drawbacks to these methods include injury to the skin and possible evisceration of the bowel between clips. This technique is credited to surgeons in Columbia who had vast experience with catastrophic abdominal trauma in the setting of limited resources. Use of a transparent closure device allows for examination of the bowel for ischemic changes. In addition, the suctioned effluent can be monitored for bloody or bilious drainage. The open abdomen may drain several liters over one day, and control of effluent with a vacuum device helps to keep the patient dry. Patients with open abdomens need not be kept paralyzed and sedated through the course of their operations. In those patients without bowel injury, enteral feeding is associated with a longer duration of open abdomen but significantly improves fascial closure rates, decreases complications, and decreases mortality. Primary fascial closure is performed whenever possible, as long as it is performed in a tension-free fashion. Earlier returns to the operating room are associated with increased rates of successful closure and decreased intra-abdominal complications. Finally, those patients whose abdomens are closed within a week, report higher quality of life, improved emotional health and are more likely to return to work than those closed after a week. A black sponge is placed over the white sponge with an occlusive dressing and the vacuum is placed to suction. This addresses the need to keep the fascia under tension to prevent fascial retraction and loss of domain. The patient is returned to the operating room every other day to perform sequential fascial closure with interrupted no. This method accepts a very high likelihood of ventral hernia in favor of temporarily closing the abdomen.
Best purchase for repaglinide
Examination of the anterior chamber should be performed looking for hyphema diabetes symptoms type 3 discount repaglinide 2 mg on line, hypopyon (layering of white cells inferiorly diagnostic of endophthalmitis in the setting of trauma), a shallow anterior chamber suggestive of open globe, an anterior chamber foreign body, and anterior chamber cell (white cells in the anterior chamber-are seen in endophthalmitis or traumatic iritis). Examination of the iris should be performed looking for iris tears or iris dialyses. Finally, examination of the lens should be performed to determine whether it is present or not (it may have been lost in the case of a corneal laceration with extrusion of ocular contents or in the case of rupture at the site of prior cataract surgery with extrusion of the intraocular implant), whether it is subluxed, whether there is an intralenticular foreign body, or whether cataractous changes have developed. Intraocular pressure is best measured using a Goldmann applanation device used with the slit lamp, but a Tono-Pen is a convenient device for use in the emergency room setting. A high pressure can be seen with hyphema or with a retrobulbar hemorrhage (due to transmission of the elevated intraorbital pressure), while a low pressure is seen with an open globe or severe intraocular inflammation. It should be noted, however, that the intraocular pressure may on occasion be normal (rarely high) with an open globe. However, a direct ophthalmoscope can establish whether the view is clear or not (if not, either there is a problem with the cornea, anterior chamber, or lens or there is a vitreous hemorrhage), can detect a choroidal rupture and commotio retinae, or can document a normal posterior pole examination. Any patient with a vitreous hemorrhage needs indirect ophthalmoscopy for detection of retinal tears or peripheral retinal detachment. Ancillary Studies B-mode ultrasonography is very useful for examination of the posterior segment in the presence of media opacities not allowing ophthalmoscopy. It should be noted that the investigation is strongly operator dependent and that even in experienced hands severe vitreous hemorrhage cannot be reliably distinguished from a retinal detachment. Chapter 20 Eye 405 Initial Management of the Patient with Ocular Trauma After the patient is stabilized (ie, life-threatening injuries have been stabilized) other organ-threatening injuries need to be managed in parallel to evaluating the injured eye. Rule out a chemical injury by history (splash of liquid into the eye, explosion at chemical facility, firework injury). If there is suspicion of a chemical injury, a pH strip should be checked (from the fornix) and irrigation should be started at once (see section "Chemical Injury"). Rule out an open globe if possible: look for the specific signs (corneal/scleral laceration, prolapse of uveal tissue, hemorrhagic chemosis of the conjunctiva, low intraocular pressure, asymmetry in anterior chamber depth, vitreous hemorrhage). If there is reasonable suspicion of an open globe, exploration in the operating room should still be carried out (such as appendectomy; while one endeavors to reduce the rate of negative exploration, it is better to have a negative exploration than to miss the diagnosis). The patient needs urgent (as soon as possible and certainly within 12 hours) repair in the operating room by an ophthalmologist-the necessary arrangements need to be made (this may include transfer to a center with an operating microscope and available ophthalmologist, ophthalmology consult, etc. Place a shield to cover the eye and instruct the patient not to squeeze his or her lids or strain as this may cause further extrusion of intraocular contents; if a metal shield is not available, a cut Styrofoam cup may be taped over the eye. When taping the shield, it is important that the edge of the shield is secure over the orbital rim (ie, make sure it is not pressing against the globe). Repair of lid lacerations or orbital fractures should never be undertaken before an open globe has been ruled out or repaired. Identify other orbital or ocular injuries and treat accordingly (see section "Specific Injuries and their Management").
Order 2 mg repaglinide fast delivery
Typical draping for trauma laparotomy should be performed with exposure from chin to knees blood sugar emergency order cheapest repaglinide and repaglinide. Anesthesia is allowed access the head and arms while the surgeon maintains access to the neck, chest, abdomen, bilateral groins, and saphenous veins. In the clearly exsanguinating patient, sterility remains desirable, but is not essential. In the relatively stable patient, prophylactic antibiotics should be given prior to incision, and a proper time-out should be performed. Role of the Surgeon During a trauma laparotomy, the surgeon plays many different roles that must be quickly integrated. They conduct the operation with the core mission as primary objective and have a plan on how to achieve it, but always with a high index of suspicion for associated injuries and occult sources of hemorrhage. The surgeon must physically perform the operation in a technically proficient manner while supervising the other members of the team. Attention to the fine details of the case as well as to big-picture physiology of the patient is necessary. Early on, a decision must be made regarding the operative profile of the case: specifically whether to perform damage control or a definitive repair, and the sequence of operative priorities. It is a concerted effort from the surgeon, the anesthesiologists, the nurses, the blood bank, and others. For the operation to be a success, continuous dialogue must be maintained amongst the entire team regarding the broad picture of what is being done and how the plan is evolving. The anesthesiologists should keep the operating surgeon updated on hemodynamics and volume status, dysrhythmias, and need for vasopressors, as well as on the presence of acidosis, coagulopathy, and hypothermia. It is with these variables of physiologic reserve that the surgeon must make critical decisions regarding the operative profile. Likewise, the patient may be bleeding from another visceral cavity, for example hemorrhaging from a chest tube, and this may be only noted by those away from the operative field. In turn, the surgeon must communicate with anesthesia upon opening the abdomen with potential release of tamponade, the presence of massive bleeding, and regarding the clamping and unclamping of major vessels which may alter hemodynamics and arterial pH. These examples illustrate that a safe operation necessitates open communication lines between the surgeon and the anesthesiologist across the sterile drapes. When a technical challenge arises that requires more specialized assistance, the appropriate thing to do is to call for help. The decision to stop and call for additional help often reflects sound judgment, humility, and ultimately puts patient safety in utmost regard.
Brant, 65 years: Cost efficient and efficacious coordination of resources is a defining characteristic of an effective trauma system. Ocular examination for trauma; clinical ultrasound aboard the International Space Station. The process is designed to guide assessment of an individual patient and is not intended as a triage tool to be used in a situation involving mass casualties or disaster.
Ugrasal, 21 years: State and local agencies instituted prehospital care systems to deliver patients to major hospitals where appropriate care could be provided. Different measures are taken to ensure safety of plasmaderived factor concentrates, including selection of healthy donors, screening donations for the absence of relevant infectious blood-borne viruses, and screening for viral markers by serologic and nucleic acid testing. Penetrating wounds of the thoracic outlet can produce combinations of injuries involving the azygous vein, innominate artery, trachea or bronchus, and superior vena cava.
Jensgar, 22 years: Efficacy of antimicrobialimpregnated external ventricular drain catheters: a prospective, randomized, controlled trial. Mass-casualty drills must include three phases: preparation phase, exercise management phase, and patient treatment phase. The Pettersson score correlates well to function37 but is only able to diagnose late arthropathic changes.
Larson, 62 years: Bacillary Angiomatosis Osteomyelitis Bacillary angiomatosis is a multisystem infectious disease caused by two closely related organisms: Bartonella henselae and Bartonella quintana. A guidewire is passed through the needle into the pleural cavity using the Seldinger technique. Even in the patient with adequate crossover flow, every attempt should be made to keep the patient normotensive with a 100% oxygen saturation level.
Corwyn, 28 years: The mediastinal pleura widely opened exposing the esophagus which is mobilized by blunt dissection. Knees and ankles are the most frequently affected joints, although wrists and small joints of the hands may also be involved. It may be defined as a usually transient alteration of neurological function caused by nonpenetrating injury to the brain and characterized by normal imaging studies.
Kliff, 53 years: Nonsurgical treatment of osteonecrosis of the femoral head includes refraining from weight bearing on the affected joint, use of analgesic and anti-inflammatory medications, and physiotherapy. Nonoperative management reduces the overall mortality of grades 3 and 4 blunt liver injuries. Limbal ischemia appears as blanching of normal conjunctival and limbus blood vessels.
Mirzo, 60 years: When such injuries are detected, treatment options are many, including operative revascularization, antiplatelet therapy and observation, and the application of covered stent grafts. Derbekyan V, NovalesDiaz J, Lisbona R: Pancoast tumor as a cause of reflex sympathetic dystrophy. It is then either stored intracellularly and eventually excreted through the feces or absorbed via ferroportin transfer out of the enterocyte, aided by ferroxidase activity of the ceruloplasmin homologue, hephaestin.
Jens, 26 years: In addition, some studies indicate it may contribute to airway obstruction and difficult intubations. Proximal interphalangeal, metacarpo phalangeal, wrist, elbow, ankle, and knee joints are most frequently affected. Hemodynamically unstable patients should be resuscitated prior to imaging according to accepted guidelines and recommendations, with some exceptions for imageguided endovascular hemostasis in select scenarios.
Leif, 50 years: Crystals using polarized light microscopy � + Inflammatory arthritis not due to crystals Gout or pseudogout Gram stain and/or culture positive The balance between adipogenesis and osteogenesis has been targeted as a potential site for the treatment of osteonecrosis. Definitive histopathologic investigations of primary aortic branch vessels have not been undertaken.
Cruz, 30 years: Most trauma centers administer fibrinogen dosed by 10 unit pools (1 fibrinogen "pack" = 10 pooled units). Etomidate decreases cerebral blow flow and cerebral metabolic demand while preserving cerebral perfusion pressure. Both laryngeal lowering and bilateral lung elevating procedures may be necessary with gaps in the trachea exceeding 5�6 cm.
Temmy, 35 years: Another valid pause in the operation exists after exploring the abdomen and finding a large retroperitoneal hematoma, allowing time to consider other operative approach options, including angiography. Prospective multicenter trial of esophageal Z-stent placement for malignant dysphagia and tracheoesophageal fistula. Okazaki K, et al: Autoimmune-related pancreatitis is associated with autoantibodies and a Th1/Th2-type cellular immune response.
Mazin, 33 years: If associated injuries require it, warfarin prophylaxis is also reasonable beginning approximately 1 week after injury. An evidence-based prehospital guideline for external hemorrhage control: American College of Surgeons Committee on Trauma. Internal validation of predictive models: efficiency of some procedures for logistic regression analysis.
Cole, 37 years: Ultrasound guidance improves the success rate of internal jugular vein cannulation. Use of three-dimensional computerized tomography reconstruction in complex facial trauma. Eight minutes or less: does the ambulance response time guideline impact trauma patient outcome
Keldron, 61 years: The tourniquet should be left uncovered so that the site can be seen and monitored for recurrent hemorrhage. The knee, hand, wrist, elbow, and shoulder are most frequently involved; hand and wrist involvement distinguishes this from other fungal arthritides. Antimicrobial prophylaxis for surgery: An advisory statement from the National Surgical Infection Prevention Project.
Wenzel, 24 years: Films of the thoracic and lumbar spine are usually obtained as separate sets of frontal and lateral projections. No clinical features specific to synovial sarcoma distinguish it from other sarcomas. It notably affects the second and third metacarpophalangeal joints but also the proximal interphalangeal joints, wrists, elbows, shoulders, and hips.
Rozhov, 36 years: The association between inflammatory myopathy and cancer is well described in adults, although the pathophysiologic mechanisms underly ing the association remain elusive. Before preparing to close fascia, the surgeon should perform a thorough search of the peritoneum for laparotomy pads and instruments. A sub-xiphoid port is placed for retraction of the liver, and a port is placed laterally on the left side just below the costal margin.
Campa, 25 years: Information about the mechanism of injury should be obtained from prehospital personnel. Nonrheumatic causes of joint pain and swelling should also be ruled out, such as septic arthritis, benign or malignant tumors, reactive arthritis, foreign body synovitis, pigmented villonodular synovitis, arterial-venous malformation, bleeding disorders (such as hemophilia), or bony fractures, including nonaccidental injury. Estimates based on more than 20 deaths may also be unstable due to high relative variability of case-level costs.
10 of 10 - Review by K. Ivan
Votes: 211 votes
Total customer reviews: 211