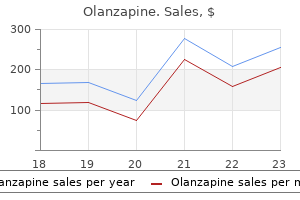
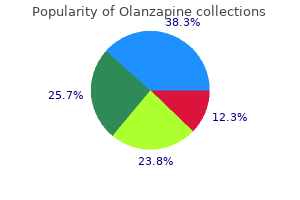
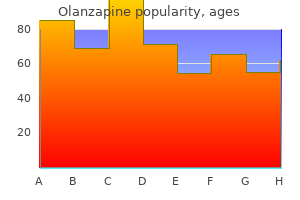
Olanzapine
Olanzapine dosages: 7.5 mg, 5 mg, 2.5 mg
Olanzapine packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Cheap olanzapine 2.5 mg buy on line
Patients with severe hemophilia have spontaneous bleeds alternative medicine buy olanzapine 5 mg visa, frequently into joints, leading to crippling arthropathies. Intracranial bleeding, intramuscular hematomas, retroperitoneal hematomas, and gastrointestinal, genitourinary, and retropharyngeal bleeding are added clinical sequelae seen with severe disease. Patients with moderately severe hemophilia have less spontaneous bleeding but are likely to bleed severely after trauma or surgery. Mild hemophiliacs do not bleed spontaneously and have only minor bleeding after major trauma or surgery. Since platelet function is normal in hemophiliacs, patients may not bleed immediately after an injury or minor surgery as Fibrinolysis Fibrin clot breakdown (lysis) allows restoration of blood flow during the healing process following injury and begins at the same time clot formation is initiated. Fibrin polymers are degraded by plasmin, a serine protease derived from the proenzyme plasminogen. Fibrinolysis is directed by circulating kinases, tissue activators, and kallikrein present in vascular endothelium. At times, the diagnosis of hemophilia is not made in these patients until after their first minor procedure. In general, activity levels should be restored to 30% to 40% for mild hemorrhage, 50% for severe bleeding, and 80% to 100% for life-threatening bleeding. For patients undergoing elective surgical procedures, a multidisciplinary approach with preoperative planning and replacement is recommended. Prothrombin complex concentrates can be used to treat deficiencies of prothrombin or factor X. The most common bleeding manifestations involve easy bruising and mucosal bleeding, particularly epistaxis or oral mucosal bleeding. The latter is important for normal platelet adhesion to exposed subendothelium and for aggregation under high shear conditions. Spontaneous bleeding is rare, but bleeding may occur after surgery, trauma, or invasive procedures. Umbilical stump bleeding is characteristic, and there is a high risk of intracranial bleeding. Significant bleeding in homozygotes with less than 1% of normal activity is encountered. The major surface protein abnormalities are thrombasthenia and Bernard-Soulier syndrome. It may be an isolated defect or occur with 90 partial albinism in the Hermansky-Pudlak syndrome.
Diseases
- Hydroxymethylglutaric aciduria
- Morphea, generalized
- Ruvalcaba Churesigaew Myhre syndrome
- Prolactinoma, familial
- Arteritis
- Frontometaphyseal dysplasia
- Curtis Rogers Stevenson syndrome
Order olanzapine with amex
For example medications john frew buy olanzapine us, in 1995, a report of the International Islet Transplant Registry indicated that of 270 recipients, only 5% were insulin-independent at 1 year posttransplant. In 2000, Shapiro and colleagues reported the results of the Edmonton protocol, which enabled consistent diabetes reversal and short-term (<1 year) insulin independence. Those results were replicated at other experienced transplant centers,112,113 but the rates of long-term (>5 year) insulin independence remained poor, well below those of whole-pancreas transplants. In fact, at 9 years posttransplant, 15% remained insulinindependent, and 73% had hypoglycemia awareness and corrected hemoglobin A1c levels. In contrast, since 2001, it has been considered a standard of care and is fully reimbursed in Canada and, more recently, in the United Kingdom, Sweden, Switzerland, France, and Italy as well. Worldwide, since 2000, more than 750 patients with diabetes have undergone an islet transplant, and 80 ongoing trials have enrolled up to 1500 islet recipients. The full potential of islet transplants remains to be realized, but the future is exciting. As the latest improvements in pancreas preservation, islet isolation and purification, islet culture, and islet immunoisolation are implemented clinically, the hope is that sustained insulin independence will become consistently possible with a single pancreas donor and without the need for systemic immunosuppression. But breakthroughs in immunosuppression, surgical technique, organ preservation, anesthesia, and critical care have improved that rate to approximately 85% today. Liver transplants remain daunting, especially in the face of an organ shortage that results in sicker potential candidates. Unfortunately, the perioperative mortality rate and the 1-year mortality rate are among the highest of any surgical operation currently performed. History the first experimental liver transplants in dogs are often attributed to C. However, current scholarship reveals that Vittorio Staudacher first described the technique in 1952. The first human liver transplant trials started in 1963 with Thomas Starzl, but a series of deaths led to a voluntary moratorium for 3. With the resumption of clinical transplants in 1967, Starzl performed the first successful liver transplant. Donor procurement techniques and cold organ preservation protocols were standardized, and the recipient operation was also refined. Choledochocholedochostomy or choledochojejunostomy to a Roux-en-Y limb became standard and significantly decreased the frequency of biliary complications. Innovations, including living donor liver transplants and deceased donor split-liver transplants, enabled more pediatric recipients to be transplanted.
Buy olanzapine 2.5 mg amex
The principles of vascular repair techniques (discussed previously) apply to carotid injuries medicine 7253 discount 7.5 mg olanzapine with amex, and options for repair include end-to-end primary repair (often possible with mobilization of the common carotid), graft interposition, and transposition procedures. All carotid injuries should be repaired except in patients who present in coma with a delay in transport. Prompt revascularization of the internal carotid artery, using a temporary Pruitt-Inahara shunt, should be considered in patients arriving in profound shock. Otherwise, carotid shunting should be done selectively as in elective carotid endarterectomy but the patient should be systemically anticoagulated. Tangential wounds of the internal jugular vein should be repaired by lateral venorrhaphy, but extensive wounds are efficiently addressed by ligation. However, it is not advisable to ligate both jugular veins due to potential intracranial hypertension. Although exposure from an anterior approach can be accomplished by removing the anterior elements of the bony canal and the tough fascia covering the artery between the elements, typically the most efficacious control of such injuries is angioembolization. Fogarty catheter balloon occlusion, however, is useful for controlling acute bleeding if encountered during neck exploration. Grade I: irregularity of the vessel wall, dissection/intramural hematoma with <25% luminal stenosis. The types of antithrombotic treatment appear equivalent in published studies to date, and the duration of treatment is empirically recommended to be 6 months. Thrombosis of the internal jugular veins caused by blunt trauma can occur unilaterally or bilaterally and is often discovered incidentally, because most patients are asymptomatic. Common injuries include thyroid cartilage fractures, rupture of the thyroepiglottic ligament, disruption of the arytenoids or vocal cord tears, and cricoid fractures. Associated injuries of the esophagus are common in penetrating injuries due to its close proximity. The sternocleidomastoid muscle or strap muscles are useful for interposition and help prevent postoperative fistulas. The most common injuries from both blunt and penetrating thoracic trauma are hemothorax and pneumothorax. The indications for thoracotomy include significant initial or ongoing hemorrhage from the tube thoracostomy and specific imaging-identified diagnoses Table 7-10). Great Vessels Over 90% of thoracic great vessel injuries are due to penetrating trauma, although blunt injury to the innominate, subclavian, or descending aorta may cause a pseudoaneurysm or frank rupture.
Olanzapine 2.5 mg purchase fast delivery
However 897 treatment plant rd generic olanzapine 5 mg buy on line, burn patients often have elevated erythropoietin levels, and a randomized study in burn patients showed that recombinant human erythropoietin did not effectively prevent anemia or decrease the number of transfusions given. Direct injury to the upper airway causes airway swelling that typically leads to maximal edema in the first 24 to 48 hours after injury and often requires a short course of endotracheal intubation for airway protection. Combustion products found in smoke, most commonly from synthetic substances in structural fires, cause lower airway injury. These irritants cause direct mucosal injury, which in turn leads to mucosal sloughing, edema, reactive bronchoconstriction, and finally obstruction of the lower airways. Injury to both the epithelium and pulmonary alveolar macrophages causes release of prostaglandins, chemokines, and other inflammatory mediators; neutrophil migration; increased tracheobronchial blood flow; and finally increased capillary permeability. Inhalation injury decreases lung compliance70 and increases airway resistance work of breathing. Since severe inhalation injury may result in mucosal sloughing with obstruction of smaller airways, bronchoscopy findings including carbon deposits, erythema, edema, bronchorrhea, and a hemorrhagic appearance may be useful for staging inhalation injury. Furthermore, bronchoalveolar lavage within 24 hours after an inhalation injury demonstrates a high rate of positive quantitative cultures,73 suggesting that pneumonia develops soon after the acute lung injury. Aggressive pulmonary toilet and routine use of nebulized bronchodilators such as albuterol are recommended. Nebulized N-acetylcysteine is an antioxidant free radical scavenger designed to decrease the toxicity of high oxygen concentrations. Aerosolized heparin aims to prevent formation of fibrin plugs and decrease the formation of airway casts. These agents seem to improve pulmonary toilet but have no demonstrated effect on mortality. Administration of intrabronchial surfactant has been used as a salvage therapy in patients with severe burns and inhalation injury. A similar approach had previously been shown to improve outcomes in pediatric burn patients. Silver sulfadiazine has a wide range of antimicrobial activity, primarily as prophylaxis against burn wound infections rather than treatment of existing infections. It has the added benefits of being inexpensive and easily applied and has soothing qualities. It is not significantly absorbed systemically and thus has minimal metabolic derangements. Silver sulfadiazine has a reputation for causing neutropenia, but this association is more likely due to neutrophil margination from the inflammatory response. True allergic reactions to the sulfa component of silver sulfadiazine are rare, and at-risk patients can have a small test patch applied to identify a burning sensation or rash. Silver sulfadiazine destroys skin grafts and is contraindicated on burns or donor sites in proximity to newly grafted areas. Also, silver sulfadiazine may retard epithelial migration in healing partial-thickness wounds. Mafenide acetate, either in cream or solution form, is an effective topical antimicrobial.
Elemi. Olanzapine.
- Dosing considerations for Elemi.
- Are there safety concerns?
- Stomach conditions and coughs.
- How does Elemi work?
- What is Elemi?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96441
Buy genuine olanzapine line
The main obstacle is the high immunogenicity of the intestine medicine to stop contractions best order olanzapine, caused by its abundant lymphoid tissue. High levels of immunosuppression are needed, yet the rejection rate is still high. Over the last several years, improvements in surgical techniques, in perioperative and postoperative care, and particularly in immunosuppressive protocols have led to significantly better patient and graft survival rates posttransplant. The definition of intestine failure does not specify the exact length of the remaining intestine. Variables include what part of the small intestine is absent, whether or not the ileocecal valve is present, whether or not the patient underwent an ostomy, and how long the remaining colon is. The disease involvement of organs other than the intestine dictates the extent of the operation required. If pathologic or biochemical evidence of severe liver damage is combined with signs of portal hypertension, then a combined liver-intestine transplant is the treatment of choice. However, a multivisceral transplant (liver, pancreas, stomach, duodenum, and/or small intestine) might be necessary among children who suffer diffuse intestinal dysmotility syndromes and adults who develop diffuse portomesenteric thrombosis, extensive intra-abdominal desmoid disease encasing the main For both the donor and recipient surgery, the key decision is which organs will be transplanted. The liver, duodenum, pancreas, and small intestine-because of their close anatomic relationship-are procured en bloc. If the hepatoduodenal ligament is left intact, no biliary reconstruction is necessary, which virtually eliminates the risk of postoperative biliary complications. However, advances in surgical techniques have made the use of living donors a feasible alternative for either an isolated intestine transplant or a combined liver-intestine transplant. For an isolated intestine transplant, venous drainage is achieved via systemic or portomesenteric drainage; for a combined liver-intestine transplant or a multivisceral transplant, venous drainage is achieved via the hepatic veins. Systemic venous drainage, given its lesser technical difficulty, is preferred over portomesenteric drainage. The diversion of splanchnic flow into the systemic venous circulation can cause several metabolic abnormalities, but no hard evidence shows any negative impact clinically on the recipient. In the early postoperative period, the ileostomy enables regular endoscopic surveillance and biopsy of the intestinal mucosa. The last, but often the most difficult, part of the recipient operation is abdominal wall closure. It is especially challenging in intestine transplant recipients because they have usually undergone multiple previous procedures, resulting in many scars, ostomies, feeding tubes, and the loss of abdominal domain. To provide sufficient coverage of the transplanted organs, the use of prosthetic mesh often is necessary.
Best purchase for olanzapine
Resultant tissue injury depends on several factors treatment 02 order olanzapine on line, including solution osmolality, tissue toxicity, vasoconstrictive properties, infusion pressure, and regional anatomic properties. The true extent of the injury may be beyond the apparent external margins, and this may take days to manifest completely (longer in the case of calcium carbonate infiltrations). Treatment varies from conservative management with limb elevation to saline infiltration (for dilution) and aspiration with liposuction cannula. Cold or warm compresses should be avoided because they may add a thermal injury component to an area in which thermoregulatory mechanism are impeded due to vasoconstriction, pressure, and inflammation. Surgical intervention includes debridement of devitalized tissue and reconstruction with appropriate technique. Thermal Injury Exposure of the skin to thermal extremes disrupts its primary function as a barrier to heat loss, evaporation, and microbial invasion. The depth and extent of injury are dependent on the duration and temperature of the exposure. Briefly, the epicenter of the injury undergoes a varying extent of necrosis (depending on the exposure), otherwise referred to as the zone of coagulation, which is surrounded by the zone of stasis, which has marginal perfusion and questionable viability. The outermost area of skin shows characteristics similar to other inflamed tissues and has been designated the zone of hyperemia. Potassium chloride intravenous infiltrate in a critically ill patient on multiple vasopressors. With rewarming, the ice melts and damaged cells take up water; affected capillaries leak fluid into the interstitium. Subsequently, this edema and concomitant inflammatory process result in epidermal blistering and microvasoconstriction, propagating further tissue injury. Pink areas are superficial partial-thickness burn, whereas whiter areas are deeper burns in the dermis. A Tissue pressures that exceed the pressure of the microcirculation (30 mmHg) result in tissue ischemia. Areas of bony prominence are particularly prone to ischemia, the most common areas being ischial tuberosity (28%), trochanter (19%), sacrum (17%), and heel (9%). Tissue pressures can measure up to 300 mmHg in the ischial region during sitting and 150 mmHg over the sacrum while lying supine. Wounds are staged as follows: stage 1, nonblanching erythema over intact skin; stage 2, partial-thickness injury (epidermis or dermis)-blister or crater; stage 3, full-thickness injury extending down to , but not including, fascia and without undermining of adjacent tissue; and stage 4, full-thickness skin injury with destruction or necrosis of muscle, bone, tendon, or joint capsule. Management principles for pressure sores should include pressure relief (air mattresses and gel cushions for redistribution of pressure), systemic optimization (particularly nutritional support), and wound care. Different types of skin substitutes arise from xenograft, autologous, synthetic, and allogeneic sources. Integra is a two-layered membrane composed of a silicon layer to maintain hydration and a porous bovine collagen and chondroitin sulfate layer that provides an environment for fibroblasts, macrophages, and capillaries to lay down a vascularized collagen matrix dermal layer. The more superficial silicon layer can be removed, and an autograft can subsequently be applied.
Olanzapine 5 mg buy with amex
Extensive axillary lymph node dissection medicine 013 2.5 mg olanzapine with mastercard, the delivery of radiation therapy, the presence of pathologic lymph nodes, and obesity are predisposing factors. Patients should be referred to physical therapy at the earliest signs of lymphedema to prevent progression to the later stages. The use of individually fitted compressive sleeves and complex decongestive therapy may be necessary. The goals of reconstructive surgery after a mastectomy for breast cancer are wound closure and breast reconstruction, which is either immediate or delayed. However, if a more radical removal of skin and subcutaneous tissue is necessary, a pedicled myocutaneous flap from the latissimus dorsi muscle is generally the best approach for wound coverage. A skin graft provides functional coverage that will tolerate adjuvant radiation therapy; however, this is not preferred, because poor graft adherence may delay delivery of radiation therapy. Breast reconstruction after riskreducing mastectomy or after mastectomy for early-stage breast cancer may be performed at the same time as the mastectomy. This allows for a skin-sparing mastectomy to be performed, Reconstruction of the Breast and Chest Wall 550 which offers the best overall cosmetic outcomes. Reconstruction can proceed with an expander/implant reconstruction or with autologous tissue such as a pedicled myocutaneous flap or a free flap using microvascular techniques. In patients with locally advanced breast cancer, reconstruction is often delayed until after completion of adjuvant radiation therapy to ensure that local-regional control of disease is obtained. The expected use of postmastectomy radiotherapy should also be considered as a reason for delayed reconstruction as radiotherapy to a reconstructed breast has been reported to result in inferior cosmetic outcomes. Consideration can be made for placement of a tissue expander to allow for skin-sparing but this should be discussed with the radiation oncologist and other members of the treatment team. If chest wall coverage is needed to replace a large skin or soft tissue defect, many different types of myocutaneous flaps are employed, but the latissimus dorsi and the rectus abdominis myocutaneous flaps are most frequently used. The latissimus dorsi myocutaneous flap consists of a skin paddle based on the underlying latissimus dorsi muscle, which is supplied by the thoracodorsal artery with contributions from the posterior intercostal arteries. When the bony chest wall is involved with cancer, resection of a portion of the bony chest wall is indicated. If only one or two ribs are resected and soft tissue coverage is provided, reconstruction of the bony defect is usually not necessary, because scar tissue will stabilize the chest wall. Adjuvant chemotherapy is of minimal benefit to women with negative nodes and cancers 0. For women with hormone receptor-negative cancers that are >1 cm in size, adjuvant chemotherapy is appropriate. For special-type cancers (tubular, mucinous, medullary, etc), which are usually strongly estrogen receptor positive, adjuvant antiestrogen therapy should be advised for cancers >1 cm.
Discount olanzapine amex
The stronger the anti-inflammatory effect of the steroid compound used medicine allergic reaction purchase discount olanzapine on-line, the greater the inhibitory effect on wound healing. Steroids used after the first 3 to 4 days postinjury do not affect wound healing as severely as when they are used in the immediate postoperative period. Therefore, if possible, their use should be delayed, or alternatively, forms with lesser anti-inflammatory effects should be administered. In addition to their effect on collagen synthesis, steroids also inhibit epithelialization and contraction and contribute to increased rates of wound infection, regardless of the time of administration. Delay in the use of such drugs for about 2 weeks postinjury appears to lessen the wound healing impairment. The increased incidence of cardiovascular disease, metabolic diseases (diabetes mellitus, malnutrition, and vitamin deficiencies), and cancer, and the widespread use of drugs that impair wound healing may all contribute to the higher incidence of wound problems in the elderly. However, more recent clinical experience suggests that major operative interventions can be accomplished safely in the elderly. The results of animal studies regarding the effects of aging on wound healing have yielded contradictory results. Thus, although wound collagen synthesis does not seem to be impaired with advanced age, noncollagenous protein accumulation at wounded sites is decreased with aging, which may impair the mechanical properties of scarring in elderly patients. Low oxygen tension has a profoundly deleterious effect on all aspects of wound healing. Fibroplasia, although stimulated initially by the hypoxic wound environment, is significantly impaired by local hypoxia. Optimal collagen synthesis requires oxygen as a cofactor, particularly for the hydroxylation steps. Increasing subcutaneous oxygen tension levels by increasing the fraction of inspired oxygen (Fio2) of inspired air for brief periods during and immediately following surgery results in enhanced collagen deposition and in decreased rates of wound infection after elective surgery. The level of vasoconstriction of the subcutaneous capillary bed is exquisitely Metabolic Disorders. Diabetes mellitus is the best known of the metabolic disorders contributing to increased rates of wound infection and failure. Additionally, the large- and small-vessel disease that is the hallmark of advanced diabetes contributes to local hypoxemia. Defects in granulocyte function, capillary ingrowth, and fibroblast proliferation all have been described in diabetes. Obesity, insulin resistance, hyperglycemia, and diabetic renal failure contribute significantly and independently to the impaired wound healing observed in diabetics.
7.5 mg olanzapine with mastercard
This imbalance between cel3 lular supply and demand leads to neuroendocrine and inflammatory responses symptoms tuberculosis purchase on line olanzapine, the magnitude of which is usually proportional to the degree and duration of shock. The specific responses will differ based on the etiology of shock, as certain physiologic responses may be limited by the inciting pathology. For example, the cardiovascular response driven by the sympathetic nervous system is markedly blunted in neurogenic or septic shock. Many of the organ-specific responses are aimed at maintaining perfusion in the cerebral and coronary circulation. These are regulated at multiple levels including (a) stretch receptors and baroreceptors in the heart and vasculature (carotid sinus and aortic arch), (b) chemoreceptors, (c) cerebral ischemia responses, (d) release of endogenous vasoconstrictors, (e) shifting of fluid into the intravascular space, and (f) renal reabsorption and conservation of salt and water. Furthermore, the pathophysiologic responses vary with time and in response to resuscitation. In hemorrhagic shock, the body can compensate for the initial loss of blood volume primarily through the neuroendocrine response to maintain hemodynamics. With continued hypoperfusion, which may be unrecognized, cellular death and injury are ongoing and the decompensation phase of shock ensues. Microcirculatory dysfunction, parenchymal tissue damage, and inflammatory cell activation can perpetuate hypoperfusion. Persistent hypoperfusion results in further hemodynamic derangements and cardiovascular collapse. This has been termed the irreversible phase of shock and can develop quite insidiously and may only be obvious in retrospect. At this point, there has occurred extensive enough parenchymal and microvascular injury such that volume resuscitation fails to reverse the process, leading to death of the patient. In experimental animal models of hemorrhagic shock (modified Wiggers model), this is represented by the "uptake phase" or "compensation endpoint" when shed blood must be returned to the animal to sustain the hypotension at the set level to prevent further hypotension and death. Decreased tissue perfusion can result directly from hemorrhage/hypovolemia, cardiac failure, or neurologic injury. Decreased tissue perfusion and cellular injury can then result in immune and inflammatory responses. Alternatively, elaboration of microbial products during infection or release of endogenous cellular products from tissue injury can result in cellular activation to subsequently influence tissue perfusion and the development of shock. Neuroendocrine and Organ-Specific Responses to Hemorrhage the goal of the neuroendocrine response to hemorrhage is to maintain perfusion to the heart and the brain, even at the expense of other organ systems. The mechanisms include autonomic control of peripheral vascular tone and cardiac contractility, hormonal response to stress and volume depletion, and local microcirculatory mechanisms that are organ specific and regulate regional blood flow. The magnitude of the neuroendocrine response is based on both the volume of blood lost and the rate at which it is lost.
Nafalem, 49 years: Radiographically, a mass is usually evident, with destruction of surrounding tissue and bone. Inhalational exposure followed by the development of symptoms is associated with a high mortality rate. The first three are determined by location in various Source: Reproduced with permission from Phillips et al. Viruses Due to their small size and necessity for growth within cells, viruses are difficult to culture, requiring a longer time than is typically optimal for clinical decision making.
Tjalf, 52 years: These findings constitute a surgical emergency, and the mainstay of treatment remains wide d�bridement of the necrotic tissue to the level of bleeding, viable tissue. Orthotopic transplants require the removal of the diseased organ (heart, lungs, liver, or intestine); in heterotopic transplants, the diseased organ is kept in place (kidney, pancreas). Indeed, several studies have recently focused on identifying a gene expression profile or a molecular signature that is associated with metastasis. Human albumin administration in critically ill patients: systematic review of randomised controlled trials.
Rufus, 61 years: Individuals with dysplastic nevi have a 10% overall lifetime risk of melanoma, with tumors arising from pre-existing nevi or de novo. Cohen et al51 have shown convincingly that activated protein C is a key element, although the complete mechanism remains to be elucidated. Virtually all transections and any injury associated with significant tissue loss will require a Roux-en-Y choledochojejunostomy. Tissue oxygenation, anemia, and perfusion in relation to wound healing in surgical patients.
Yugul, 38 years: Fluid resuscitation is a major adjunct to physically controlling hemorrhage in patients with shock. Time to deterioration of the elderly, anticoagulated, minor head injury patient who presents without evidence of neurologic abnormality. Each reactor operator is aware of what is going on at all times and is responsible for understanding the implications and possible consequences of any action. Nonpulmonary thoracic symptoms result from invasion of the primary tumor directly into a contiguous structure.
Ningal, 44 years: It is important to evaluate the wound under these dressings if patient demonstrates signs of sepsis with an unidentified source, since typical clues of wound sepsis such as odor and drainage are hidden by the suction apparatus. The pectoralis myocutaneous flap has enjoyed tremendous popularity because of its ease of harvest, the ability to tailor its thickness to the defect, and limited donor site morbidity. Five clinical types are identified: ulcerative, pustular, bullous, vegetative, and peristomal. Lower-voltage, higher-wattage current (cutting current) is better for tissue desiccation and vaporization.
Gembak, 50 years: Povidone-iodine spray technique versus traditional scrub-paint technique for preoperative abdominal wall preparation. On occasion, septic patients may have low cardiac output despite volume resuscitation and even vasopressor support. The simultaneous administration of calcium gluconate will counteract the adverse side effects of a rapidly rising magnesium level and correct hypocalcemia, which is frequently associated with hypomagnesemia. Cultured skin substitutes reduce donor skin harvesting for closure of excised, full-thickness burns.
Kent, 27 years: Comparison of cooling methods to induce and maintain normo- and hypothermia in intensive care unit patients: a prospective intervention study. The final two channels are used for pressure monitoring and the injection of the thermal indicator for determinations of cardiac output. Presentation is characteristically a slowgrowing, asymptomatic, violaceous plaque involving the trunk, head, neck, or extremities. Hepatitis B immunization in children has recently been shown to reduce the incidence of liver cancer.
Jens, 34 years: Proximal control is obtained just above the iliac bifurcation with direct pressure via a sponge stick; the injury is identified by cephalad dissection along the anterior surface of the inferior vena cava. The diagnosis can be confirmed by documenting a paradoxical increase in urine osmolality in response to a period of water deprivation. In keloids, the collagen bundles are virtually nonexistent, and the fibers are connected haphazardly in loose sheets with a random orientation to the epithelium. The G1 and G2 phases represent gap phases during which the cells prepare themselves for completion of the S and M phases, respectively.
Nefarius, 26 years: Partial palatectomy of infrastructure maxillectomy may be required for larger lesions involving the palate or maxillary antrum. There are also ongoing studies on approaches to assess margins intraoperatively, to allow immediate intraoperative reexcisions as needed, and maximizing local control. Some surgeons perform mediastinoscopy in all lung cancer patients because of the poor survival associated with surgical resection of N2 disease. Effects of different plasma substitutes on blood coagulation: a comparative review.
Hjalte, 65 years: These are also useful for superficial partialthickness facial burns as they can be applied and left open to air without dressing coverage. Repeat as needed, depending on fibrinogen level, and request appropriate amount of cryoprecipitate. In 1948, Stewart and Treves described lymphangiosarcoma of the upper extremity in women with ipsilateral lymphedema after radical mastectomy. Sodium chloride is an ideal solution, however, for correcting volume deficits associated with hyponatremia, hypochloremia, and metabolic alkalosis.
Spike, 47 years: The goals of therapy include reducing the total body potassium, shifting potassium from the extracellular to the intracellular space, and protecting the cells from the effects of increased potassium. The level of vasoconstriction of the subcutaneous capillary bed is exquisitely Metabolic Disorders. Finally, the breast and axillary contents are removed from the surgical bed and are sent for pathologic assessment. It turns over continuously, regulated by mechanisms controlling the synthesis and degradation of its protein components.
8 of 10 - Review by H. Norris
Votes: 319 votes
Total customer reviews: 319