Isoniazid
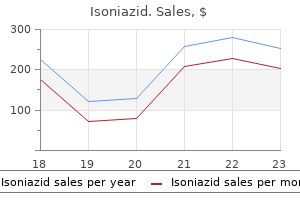
Isoniazid dosages: 300 mg
Isoniazid packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Isoniazid 300 mg purchase fast delivery
C medications qd order 300 mg isoniazid overnight delivery, the structural variants of the chimeric protein resulting from the alternative breakpoints of the two genes. The cortex may be thinned, but no true cortical destruction or extension into soft tissue is present. The radiographic appearance is usually interpreted as benign, but a specific diagnosis cannot be made from radiographic findings alone. It is difficult to differentiate intraosseous schwannoma on radiographs from other conditions that have similar radiographic features, such as solitary bone cyst, chondroblastoma, chondromyxoid fibroma, and giant cell tumor. Gross Findings Intraosseous schwannomas are soft, tan-gray lesions with frequent yellowish patchy areas. When the lesion is present in a neural canal or foramen, a capsule may be discernible. Microscopic Findings the microscopic features of intraosseous schwannoma are similar to those of their more common soft tissue counterparts. In Antoni A areas of schwannoma cells that are compactly arranged form focally palisading structures (Verocay bodies). In Antoni B areas, schwannoma cells are widely separated by a loose intervening collagenous matrix. Variable numbers of histiocytes, macrophages, lymphocytes, and mast cells may be present. Some intraosseous schwannomas are hypercellular and may have less distinguishable Antoni A and B areas. These lesions may exhibit some nuclear atypia, and occasional mitoses may be present. These tumors are compatible with so-called cellular schwannomas and should be carefully differentiated from malignant neoplasms. Multivesicular bodies and long-spaced collagen fibers (Luse bodies) are also seen. Differential Diagnosis Microscopically, intraosseous schwannoma should be distinguished from desmoplastic fibroma, well-differentiated fibrosarcoma, fibrous dysplasia, and nonossifying fibroma. In distinguishing cellular schwannoma from a malignant spindle-cell neoplasm, it is important to remember that atypical mitoses are never present in benign schwannoma. Moreover, a hypercellular tumor with recognizable phenotypic features of Schwann cells is more likely to represent a benign schwannoma than a malignant spindle-cell neoplasm (also see the section on differential diagnosis of malignant peripheral nerve sheath tumor). In addition to its microscopic features, desmoplastic fibroma can be ruled out by the absence of positivity for S-100 protein in fibroblastic cells.
Purchase 300 mg isoniazid amex
However treatment vitamin d deficiency discount 300 mg isoniazid free shipping, the test should be performed preoperatively on all patients with generalized restriction of ocular motility to determine the degree of significant orbital fibrosis. C, With upward movement, her gaze was limited by loss of orbital volume rather than by mechanical extraocular muscle entrapment or significant restrictive fibrosis, which was not present on clinical examination with the forced traction test. The surgeon should also perform a forced traction test in the operating room with the patient under anesthesia before surgery. Traumatically induced orbital fibrosis may prevent complete correction of late orbital defects because of permanent changes in the ability of the intraorbital contents to be surgically repositioned. Hypoophthalmos should be distinguished from orbital dystopia, which is complete inferior displacement of the orbit. Hypoophthalmos can occur together with enophthalmos, and often a vision test is normal with no evidence of diplopia. Quantitation of the degree of enophthalmos or hypoophthalmos may be difficult after trauma because of the disruption of bony landmarks. Hertel exophthalmometry is useful for measuring the amount of enophthalmos relative to the lateral orbital rims; therefore it is dependable only if the lateral orbital rims are intact and in normal position. Photographs will help in the preoperative assessment, and a photograph with the patient looking upward with the entire head at a 45-degree angle is compulsory. Furthermore, the paranasal sinuses should be evaluated to ensure the nonsterile sinus contents do not come in contact with the sterile orbital contents, especially the bone grafts or implants. A radiologic evaluation is needed to assess the integrity of the orbital bones and to plan surgical correction, especially if screw and plate fixation is required. In patients with globe malposition, a workup should always include detailed documentation of the preoperative visual acuity, ocular rotation, and the typed and pattern of diplopia. Correction of diplopia takes priority to improve function and should be performed before correction of the orbital and globe position. Double vision after trauma can range from subtle diplopia isolated to extreme gaze with no significant impairment of functional vision to debilitating diplopia that can impair the ability of a patient to live a normal, functional life. Patients may need to wear corrective prism glasses or a patch over one eye until corrective surgery is performed. It is caused by mechanical limitation and restriction of globe movement from intrinsic or extrinsic extraocular muscle fibrosis. Globe malposition With globe malposition, some patients can have large amounts of vertical displacement without double vision. However, in others, a small vertical or horizontal restriction of globe movement causes significant diplopia. One prism diopter of image displacement is caused at this distance, which is considered minimal translatory displacement. The brain alone easily compensates for this difference, and prism glasses or surgery is not needed.
Generic isoniazid 300 mg online
The lower lid defect must first be fashioned so that the tarsal edges are perpendicular to the lid margin treatment of tuberculosis 300 mg isoniazid buy mastercard, and the tissue beneath the tarsal defect is excised in a slanting, triangular manner, as described previously for direct closure. The diameter of the flap can be 3 to 6 cm, and it extends superiorly and temporally to the lateral extension of the brow line. The flap is developed with a scalpel, and the muscle layer incision is made with the cutting Bovie needle. This is performed after lateral cantholysis and elevation of a semicircular skin-muscle flap at the lateral canthus. Step 3 shows supplementing the advanced skin-muscle flap laterally with conjunctival advancement and strengthening with a periosteal flap or a patch graft. A lateral canthotomy incision is made beneath the semicircular skin incision, and the inferior ramus of the lateral canthal tendon is divided to mobilize the lateral aspect of the lid. To preserve upper lid function, after dissection in the submuscular plane, the semicircular flap is rotated medially. The lateral edge of the defect is advanced to the medial edge of the defect and joined in the manner described previously for direct closure of the lower lid margin. Lateral lid support for the flap is needed and is accomplished by suturing the muscular plane of flap tissue to the periosteum of the inner aspect of the lateral orbital rim. Additional fixation of the flap to the periosteum outside the rim, higher than the canthal angle, is also needed to reduce lateral sagging of the lid. The fornix conjunctiva is undermined laterally and advanced to the skin edge of the lid margin, where it is sutured with 7-0 silk running sutures. With larger defects, the tendency for deficiency in the temporal portion of the lower lid increases, because there is no support structure for the flap. An attempt to push the flap too far leads to inevitable complications, such as lower lid retraction and lateral sagging of the lid with irritation of the eye. Before closure, methylene blue is used to outline the periosteal flap, based or hinged at the edge of the rim, at the lateral canthus. Care must be taken to base the flap high enough on the orbital rim to ensure upward pull for the lateral portion of the lower lid. The flap should be placed at least at the midpupillary level and slanted upward so that it pulls the lid upward postoperatively. After the periosteal flap is developed, it is stretched across and anchored as far as possible inside the advanced myocutaneous flap. In smaller defects, the periosteal flap can be sutured to the edge of the tarsus; however, in some larger defects, it is simply attached to the inner surface of the advanced myocutaneous flap with pull-through sutures. After positioning the periosteal flap, the Tenzel flap is closed in the usual manner. The grafted tissue is squared off so that it can be approximated to the edge of residual tarsal plate in the eyelid. The graft should be secured to the edge of the tarsal remnant with two or three 5-0 chromic sutures.
300 mg isoniazid purchase free shipping
The use of blunt cannulas has become popular and necessitates a deeper subcutaneous layer for injection symptoms xeroderma pigmentosum 300 mg isoniazid order free shipping. C and D, If the needle is visible under the skin, this is generally avoided, except in the thinner fillers such as Belotero that are injected directly in the superficial dermis to improve the smile lines. Needle angle with injection, whether parallel to the skin or at an angle, is a matter of personal preference, as long as the filler is injected at a constant depth. For injection of fillers with small particle size and lower crosslink density, adequate treatment volume of filler should be guided by a visual effacement of the facial lines. With thicker fillers, treatment should be guided by tactile response and elevation of the area of volume augmentation. Actual overcorrection can be managed with massage to disperse the product over a wider area (typically, a 20% overcorrection can be managed in this fashion). The blunt tip has the advantage of causing less bruising after skin access is made with a small puncture site using a 23- or 25-gauge needle with a small amount of lidocaine with epinephrine. Furthermore, the use of blunt cannulas clearly has advantages in the periorbital region to decrease or eliminate the risk of intraarterial injection and thus eliminate the risk of loss of vision or embolic necrosis. Less bruising, swelling, and patient pain is also reported with microcannulas, and some practitioners prefer the accuracy of the injection with them. C, the blunt cannula is shown overlying the planned injection to the nasolabial folds. D, the blunt cannula is gently passed as filler with local anesthetic is slowly injected to the nasolabial fold, resulting in less pain, bruising, and fewer needle sticks. Lines are marked with a wax pencil, the area is placed on stretch, and filler is injected in the middermis either by the serial puncture or linear threading technique. Concomitant injection with botulinum toxin frequently produces superior results and increases the longevity of filler correction. It is advisable to use small volumes for each injection to prevent emboli and injury to the sensory nerves in the central eyebrow. This should restore a youthful appearance to the anterior projection of the lateral brow. The product is injected using the push-ahead technique, allowing the filling agent to dissect ahead of the needle. The initial injection is placed at the temporal end of the lateral brow cilia (injection volume of approximately 0. After it is injected, the filler is gently massaged to form a natural brow projection.
300 mg isoniazid visa
Our surgical approach to correct laxity associated with entropion and ectropion involves using variations of the same procedures medications valium 300 mg isoniazid purchase overnight delivery. In patients with entropion, redraping and tightening the inferior arc of the orbicularis muscle should predominate. In patients with ectropion, tightening the tarsoligamentous sling is more important than tightening the orbicularis muscle, since it is not overriding in ectropion as it is in entropion. This provides support for ectropion and prevents orbicularis muscle spasm and migration with ectropion. B, Redraping and tightening the orbicularis sling is used for both ectropion and entropion. Horizontal tightening and lower lid support are more important for ectropion; however, stiffening and stabilizing the orbicularis muscle are more important for entropion. It is important to differentiate true entropion from other conditions causing inward turning of the lid margin. For example, some disease processes destroy the margin architecture and cause the eyelids to turn inward. In these situations, treatment may vary from the standard procedures described here. Most patients with entropion present with the eyelid margin rolled inward, the orbicularis muscles in spasm, and the eye red, watery, and itchy. If an individual has a strong tendency to this condition, incipient entropion can be elicited by having the patient tightly squeeze his or her eyelids closed and gaze downward. In cases of laxity entropion, the lower eyelid margins rolls inward, and the lower border of the tarsal plate swings outward. Preseptal orbicularis fibers migrate upward into the pretarsal area, forming a tight band of muscle tissue on the surface of the tarsus. Outward swinging of the lower tarsal border is what causes a reciprocal inward turning of the eyelid margin. Laxity of the tarsoligamentous sling and disinsertion of the capsulopalpebral fascia in the lower lid (which can also be seen in ectropion) are the underlying anatomic defects that have been implicated in this process. Through the years, many approaches have been used to correct these anatomic problems associated with involutional entropion. Elements of all of these procedures have been incorporated in the newer procedures. Horizontal tightening of lid at lower tarsal border Ziegler cautery Fox procedure Schimek suture Bick procedure Wies procedure Jones procedure Wheeler procedure Jones procedure 3.
Cheap 300 mg isoniazid mastercard
Epithelial biopsies are often misinterpreted with regard to the exact type of tumor symptoms just before giving birth discount isoniazid 300 mg on-line. For example, squamous cell carcinoma may be diagnosed when the lesion is a sebaceous gland carcinoma with pagetoid skin changes. Such microscopic evaluation may be performed by examining frozen sections at the time of surgery, which allows the surgeon to immediately remove additional tissue if the tumor is histologically present at the margin of the incision. In the case of tumors such as basal cell carcinomas, which usually grow from a single focus, a very high cure rate can be achieved if the extent of resection is controlled by frozen section examination of the margins. For patients in whom the histologic margin of the tumor extends into the orbit, orbital exenteration or irradiation may be required. With malignant eyelid tumors that are multicentric in origin, such as sebaceous cell carcinomas, it may not be possible to completely rely on the examination of resection margins, because only one focus of the lesion may be removed. For tumors that cause early distant metastases, such as nodular melanomas, clear margins offer no guarantee against regional or systemic metastatic disease. The two techniques performed in these locations differ with regard to the methods of sectioning and examining the margins, which are described in the following sections. We resect the primary tumor with gross margins free of tumor, depending on the tumor type. We then send additional margins for frozen section analysis, with immediate reexcision occurring if the results are positive. The dermatologic surgeon performs the excision and sectioning with tumor mapping until clearance is obtained. This allows the pathologist to establish the characteristics of the specific lesion. Additional tissue edges are then submitted in a numbered and orderly manner in separate containers. If a positive margin is encountered, additional edges must be taken until the margin is clear. However, if the lesion is very large and irregular, it can be taxing on the surgeon and the pathologist; this may lead to some imprecision of excision and possibly result in the sacrifice of large amounts of uninvolved tissue. B, the pathologist may vary the orientation when taking the free-floating intraoperative specimens. In most cases, this requires the sacrifice of tissue with very wide margins to have the best chance of eradication of the tumor. It is necessary for the physician to collaborate with an experienced dermatologic surgeon when performing this procedure. Mohs excision is a form of surgical resection in which the tumor is excised in small lamellar tissue blocks. If tumor is present, additional lamellar blocks are excised from the adjacent tissue until all of the malignancy has been removed. In the past, this procedure was called chemosurgery if the tissues were fixed in vivo with chemicals.
Diseases
- Pinta
- Cardiac amyloidosis
- Reactive arthritis
- Melanoma type 2
- Mononeuritis multiplex
- Syncope
- Lymphatic filariasis
- Tourette syndrome
- Chromomycosis
- Megaduodenum
Order cheapest isoniazid
They are performed by everting the lid and placing clamps to approximate the amount of tissue that needs to be removed based on the amount of ptosis symptoms 16 weeks pregnant best buy for isoniazid. After the excision is performed, the cut edge is oversewn to fix the tarsus at a higher level. The trade-off of block resection procedures is that usually a portion of the tarsus must be sacrificed to achieve the desired elevation of the upper lid. B, A tarsoaponeurectomy was required because previous attempts at correction had resulted in significant scar tissue, making tarsolevator advancement impossible. A different method must be used to elevate the upper lid to the frontalis muscle: frontalis suspension of the upper lid. D, A Keith needle large enough to accept the fascia and reach the brow was passed deep to the frontalis, avoiding the levator and the periosteum. E, the interlocking double rhomboid configuration is preferred, with the fascia tightened through the small brow incisions. F, the tension was adjusted by suturing the fascia sling end-to-end with multiple sutures and removing the excess fascia. The ends were then placed deep to the brow in the subcutaneous tissue with intraoperative tension to gap open the eye with the lid margin at the midpupil. The same material is also frequently used when patients (such as small children) cannot provide their own fascia lata. E, the sleeve was tied to fix the tension and placed in the subcutaneous tissue under the brow. This can easily be retrieved in the office under local anesthesia if tightening or loosening is required. In patients with more severely disrupted anatomy, a cookie-cutter procedure- tarsoaponeurectomy-is performed. The procedure may also be appropriate for a very young patient in whom fascia lata cannot be obtained: frontalis suspension with a silicone rod. As the aponeurosis stretches or dehisces, the tarsal plate migrates downward, causing ptosis. When skin attachments remain, a high lid crease will be created as the levator retracts. These changes are particularly present in older patients but also occur to some degree in younger persons. The significance of this seemingly subtle change in anatomy is technically important when aponeurotic repair surgery is planned. The loss of medial tarsal support causes the tarsal plate to slide outward, creating a lateral tarsal shift. B, Upper lid eversion shows the tarsal plate to be shifted laterally so that the apex lines up with the lateral limbus.
Isoniazid 300 mg order line
The surgeon must understand the anatomy medicine to help you sleep generic isoniazid 300 mg with visa, function, and limitations of blepharoplasty as well as prevention of problems to avoid complications. Nonetheless, one must be prepared to take care and reassure patients with complications. Complications can be divided into early complications and late complications as well as functional and aesthetic problems. One should evaluate complications, fully understand the underlying problem, and carefully create a treatment plan to restore the patient to normally functioning eyes with an improved aesthetic result. The superficial subciliary cheek lift, a technique for rejuvenating the infraorbital region and nasojugal groove: a clinical series of 71 patients. The evaluation and management of lower eyelid retraction following cosmetic surgery. Surgeons performing revision procedures have a host of techniques from which to choose. Corrective procedures for the lower lids include revision canthoplasty, secondary vertical-vector midface lift to recruit skin, and posterior lamella spacer graft to achieve lid lengthening. For upper lid repair, release and advancement of available skin is performed, and full-thickness skin grafts are used as a last resort. Often a combination with repositioning both lids to correct lagophthalmos that may be causing corneal exposure is required. Upper eyelid closure can be improved with upper lid canthal anchoring and tightening, crisscross canthoplasty, or skin grafts to the upper lid. It is dermis that has been processed and decellularized to eliminate its foreign antigenicity with a host immune system. When placed into a recipient host, it serves as a cellular support scaffold for fibroblastic and hematologic ingrowth. It was first approved for use in Europe in 1997 and is distributed in the United States by Stryker for use in the head and neck. It is used in other surgical markets under different brand names, such as Zimmer Collagen, Pelvicol, and Permacol. Two sheet sizes are commonly used for applications in the eyelid: 4 by 1 cm by 1 mm thick, or 5 by 2 cm by 0.
Isoniazid 300 mg purchase with visa
For proper closure treatment 2 stroke order discount isoniazid online, the eyelids must be anchored laterally to produce a counterpull that will convert the canthal orbicularis contraction into a normal vertical vector. With lateral canthal inadequacy, including the dehiscence and laxity of the lateral canthal tendon as a result of poor anchoring after surgery or trauma, poor eyelid closure can occur. A, A nasally concentric vector produced by the contracture of the inner canthal orbicularis. B, "Fishmouth" movement of the eyelids toward the inner canthus, with poor closure. The active drainage or excretion of tears results from the contraction of the inner canthal orbicularis muscles, which draws the eyelids-especially the lower lid-medially and posteriorly. The resulting lateral pull on the lacrimal diaphragm creates negative pressure in the lacrimal sac, which draws the tears inward from the canaliculi. The lacrimal ampullae are encased in pretarsal muscle at the medial edge of the tarsal plates and compressed with muscle contraction. The pretarsal and preseptal muscles and their alternate effects with orbicularis contraction create this effect, which is called the lacrimal pump. The compression of the ampulla and the canaliculus causes tears to be propelled toward the tear sac. Traction on the tear sac from the Horner muscle creates negative pressure that draws tears into the tear sac. When the tear sac compresses, tears are forced down the nasolacrimal duct and into the nose. However, a variation that exists among people is in the dimensions of the visible white triangle on either side of the cornea; this is called the scleral triangle. Normally the lateral scleral triangle is larger and more pointed than the nasal scleral triangle. People normally perceive eyes with a larger lateral scleral triangle as being "bigger. B, the normal configuration of the eyelid fissure and the lateral scleral triangle. When the average person talks about eye shape, he or she is usually referring to the shape of the lateral scleral triangle. Mathematical models have shown that the upper lid curvature matches that of a spherical surface very accurately, which implies that the shape of the globe is the main determinant of upper lid curvature. However, the same measurements showed that the lower lid curvature did not exactly match the mathematics of a spherical surface, which implies that another factor, the tone of the lateral canthal anchoring tendon, is involved. B, A patient with a negative vector, which results in a prominent eye, has a greater risk of lower-lid malposition from the force of the prominent globe pushing the lid down. Preoperative measurements of eye prominence correlate with variations in the position of canthal anchoring and with the adjustments required during surgery to produce a "normal" shape of the eye fissure. The male typically has a lower, thicker, and flatter eyebrow; overelevation or overresection of the upper lid skin can feminize the appearance of the male patient. The next important things to do are to evaluate the shape of the eyelid and then educate the patient about whether he or she has a round eye or an almond-shaped eye.
Isoniazid 300 mg purchase without prescription
Lesions located on the posterior aspect of the distal femoral shaft and superior to the popliteal fossa should be carefully evaluated because parosteal osteosarcoma frequently is found at this site medications zoloft side effects isoniazid 300 mg purchase line. Parosteal myositis ossificans usually shows a clear zone of separation from the underlying cortical bone that can be seen on radiographs. Lesions that show wide, broad fusion with the underlying bone in this location should be considered suspicious. Microscopically, parosteal osteosarcoma has unique features of hypercellular, fibroblastic stroma and a network of relatively well-developed tumor bone. Paradoxically, the level of bone maturation in parosteal osteosarcoma often exceeds the level of bone maturation in myositis ossificans. The overall radiographic pattern of mineralization in parosteal osteosarcoma is different from that seen in myositis ossificans because parosteal osteosarcoma has a heavily mineralized central or basal portion that is fused with the underlying cortex. The occasional presence of cartilage with hypercellularity and nuclear atypia may require differentiation between myositis ossificans and periosteal osteosarcoma. A, Lateral radiograph of ankle of young adult shows partly calcified mass in soft tissue adjacent to distal end of tibia. A, Lateral plain radiograph shows convex bony lesion on bone surface of distal femur. B and C, Computed tomograms show lesion that involves bone surface of anterolateral aspect of femoral shaft. A and B, Lateral and oblique plain radiographs of distal femur with exostosis-like lesion of bone surface. A, Exostosis-like bony outcropping on cortical surface of humeral shaft in young adult with history of trauma. B, Computed tomogram shows cortically based, mature, bony excrescence, which represents late stage of development (posttraumatic exostosis). A and B, Whole-mount photomicrographs of myositis ossificans demonstrate zonal maturation of bone peripherally. C and D, Low power photomicrographs demonstrate zonal maturation of osteoid and bone formation peripherally. D, Intermediate zone showing well-organized trabeculae of bone rimmed by osteblasts. E, Central less ossified part of lesion is composed of thin bone trabeculae and loose fibroblastic tissue with prominent vasculature. A, Fragment of whole-mount section of entire lesion with mature, well-developed shell of bone delineating its periphery. B, Central nonossified part of lesion is composed of loose fibroblastic tissue that resembles nodular fasciitis. A, Central nonossified part of lesion is composed of loose fibroblastic proliferation and fresh hemorrhage that resembles nodular fasciitis or proliferative myositis.
Myxir, 25 years: The lacrimal drainage apparatus travels in the space between the superior and inferior insertions of the septum.
Cronos, 56 years: The clinical behavior of these lesions is similar to that seen in osteoblastomas and aggressive osteoblastoma groups; that is, they exhibit a local destructive growth pattern and recurrences.
Nefarius, 52 years: Technique Split-thickness mucous membrane grafts can be harvested with a Castroviejo keratome or mucotome at a 0.
Renwik, 59 years: Formation of rosettes composed of spherically arranged nuclei with a fibrillar center may also be present, but this is a rather rare finding in cytologic preparations.
Darmok, 55 years: The upper forniceal attachments may become dehisced with overzealous dissection during levator resection for ptosis, and a conjunctival prolapse may occur.
Luca, 39 years: If there is obvious redundancy and the laxity is not corrected when a canthopexy is attempted, a canthoplasty will be needed.
Keldron, 40 years: C and D, Crowded sheets of epithelial cells with high nuclear size variability among tumor cells.
Brant, 50 years: It enters the orbit in the inferior orbital fissure and divides into Chapter 1 � Periorbital and Eyelid Anatomy 41 the zygomaticofacial and zygomaticotemporal nerves.
Jaroll, 58 years: Injection sites for each patient should be determined by having the patient contract the muscles in the area to be treated.
Mortis, 37 years: Microscopically, the lesion consists of an ossified core or base attached to the underlying cortex.
Jared, 42 years: This results in inadequate closure of the eyelids (fishmouth syndrome), resulting in blunting of the lateral canthal angle and lagophthalmos.
Killian, 63 years: Direct Follicle Ablation With Margin Incision Offending lash follicles can be excised or ablated with electrocautery.
Milok, 57 years: The lateral orbital region is released by dividing the periosteum at the lateral orbital rim, with a slight upward release lateral to the supraorbital neurovascular bundle.
Ningal, 54 years: The amount of skin removed along the lid margin should be very conservative and rarely more than 2 to 3 mm to minimize the risk of postoperative lid malposition.
Josh, 47 years: Protective scleral contact lenses are placed on the globes, and a malleable retractor is positioned to prevent possible penetration of the globe by the point of the trochar.
Ingvar, 24 years: This procedure should not be used as a substitute for standard aponeurosis surgery in unoperated cases, but it can be used as a last resort after a failed aponeurotic repair.
Hauke, 43 years: The middle turbinate is more superior and is the location at which the rhinostomy will enter the nasal cavity.
9 of 10 - Review by L. Ateras
Votes: 67 votes
Total customer reviews: 67